
Two Conditions That Are Often Misdiagnosed as Carpal Tunnel Syndrome

Key Takeaway
Cervical radiculopathy (pinched nerve in the neck) and rheumatoid arthritis (autoimmune attacks of the joints of hands and wrists) are the two most common conditions that are confused with carpal tunnel syndrome. Both are different causes as all three result in loss of sensation in hands, tingling and weakness. The simplest of the facts to remember: carpal tunnel symptoms are felt in the wrist, the thumb-side fingers and are worse at night; cervical radiculopathy is felt in the neck and shooting down the arm; and rheumatoid arthritis affects multiple joints symmetrically and is worse in the morning. If a regular cts treatment is not effective, then it may be time to get a second opinion.
You get the splint. Worn at night. Perhaps you receive the cortisone injection. Nor will the numbness in your hand ever go away. It’s a point that gets brought up again and again for a frustrating amount of folks: The issue wasn’t really carpal tunnel syndrome to begin with.
Carpal tunnel is one of the more frequent complaints of pain in the hand that brings individuals to a doctor’s office but “numb tingly hand” is not a diagnosis. It’s a symptom of a few entirely different conditions and two of them are referred to as carpal tunnel enough to warrant their names.
What Is Carpal Tunnel Syndrome?
Carpal tunnel syndrome happens when the median nerve gets compressed where it passes through a narrow channel at the base of the wrist. The reason why the carpal tunnel is such a small, tight space that’s surrounded by small wrist bones on three sides, and a tough band of ligament on top. The median nerve is cramped there with nine tendons, so there’s not a lot of room to spare. Anything that takes up less room or pushes the tissue against the nerve causes the nerve to be compressed.
The result is a fairly specific symptom pattern: numbness and tingling in the thumb, index, middle, and half of the ring finger, often worst in the middle of the night, sometimes with a weak grip or a tendency to drop things. A classic tell is the “flick sign” shaking the hand out brings pain relief. According to the National Institute of Neurological Disorders and Stroke, the condition is frequently linked to repetitive motion, wrist anatomy, and health conditions like diabetes, thyroid disorders, and pregnancy.
This is the genuine article. The problem is that a number of other conditions mimic it closely enough that it leads people to the wrong treatment. The point of this is not academic – a carpal tunnel release will not help with a pinched nerve in the neck, and a wrist splint will not help with the autoimmune joint inflammation in the wrist. React to the wrong issue and end up losing months and the real issue continues to fester.
1. Cervical Radiculopathy
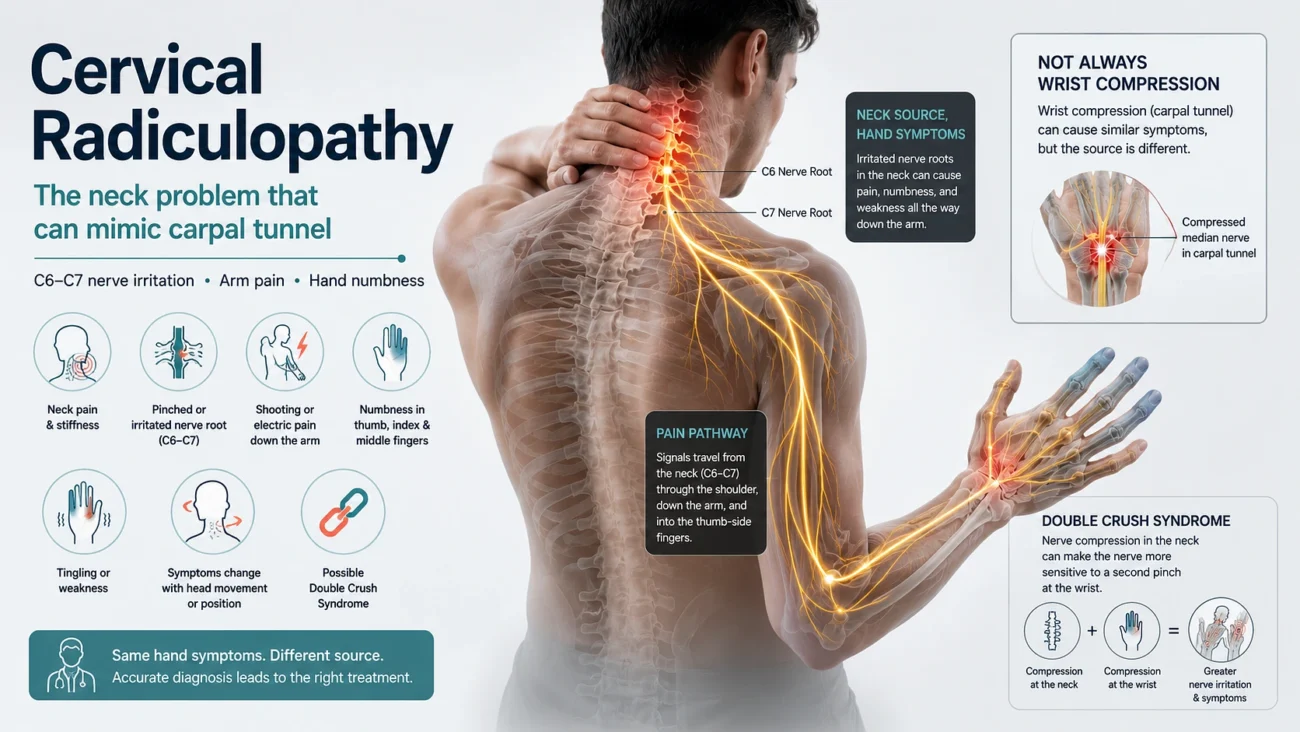
This is the impostor that fools almost everyone, because the symptoms land in your hand even though the trouble starts much higher up.
Cervical radiculopathy occurs when a nerve root is compressed or irritated when it passes from the spine in your neck. These are typically due to a herniated or bulging disc, a narrowing of the spinal canal or just arthritic deterioration of the cervical vertebrae. When that nerve root is compressed, it may send pain, numbness, tingling and weakness down the arm, into the fingers. The Cleveland Clinic mentions symptoms can spread down the length of the injured nerve.
Here’s the part that creates real diagnostic chaos: the C6 and C7 nerve roots in your neck happen to feed sensation to the thumb, index, and middle fingers the exact same fingers the median nerve serves. So a neck problem and a wrist problem can produce a nearly identical map of numb fingers. A cross-sectional study published in the National Library of Medicine confirms that impairment in the C6 and C7 roots produces overlapping signs with carpal tunnel and is a recognized source of misdiagnosis. Finger numbness alone genuinely cannot tell the two apart.
What makes it special: The clues are above the wrist. Neck pain, stiffness, or a significant decrease in neck motion with strong head turning, is not seen in cervical radiculopathy, but is seen in carpal tunnel. The pain is also different; rather than dull ache and typical “pins and needles” during the night that are characteristic of carpal tunnel, the pain is sharp, shooting or electric, down the arm and into the shoulder. That’s a useful cue, if the sensation of your hand changes when you turn or tilt your head. Most cases don’t mention their stiff neck because that’s something that goes unnoticed. If the doctor doesn’t ask, it does not come up.
There’s also a complication worth knowing about. The two conditions aren’t mutually exclusive a meaningful share of patients have both at once, sometimes called double crush syndrome, where a nerve compressed up at the neck becomes more vulnerable to a second pinch at the wrist. Which is exactly why fixing one site doesn’t always clear every symptom.
2. Rheumatoid Arthritis

The second common substitute is rheumatoid arthritis and it’s another look-alike. RA is a systemic autoimmune disease: the immune system sets its sights on the lining of the joints, aiming at the small ones of the hands and wrists in particular.
The carpal tunnel link is virtually mechanical. With RA, the inflammation and swelling of the tissue around the wrist joint fill up space, and the median nerve, nested between a narrow opening, is squeezed by the swelling. So, under the surface, RA can cause real carpal tunnel symptoms, just as it can on the surface. According to the Arthritis Foundation, RA is a chronic inflammatory condition that typically affects the hands and wrists. The wear and tear type of osteoarthritis can also squeeze the wrist this way, but typically it is RA that leads to a misdiagnosis.
How to know: Nature of pain. Carpal tunnel keeps disciplined and remains within the territory of the median nerve in one hand. RA spreads. It typically involves multiple joints, and often occurs in both hands simultaneously (bilateral). Also, the timing is an indicator—the stiffness in the joints isn't related to nerves, and it's there when you wake up, and doesn't subside rapidly. Other symptoms not related to the hands are tiredness, feeling ill, and occasionally low-grade fever. Carpal tunnel doesn't do any of that. If, in the presence of hand symptoms, there are signs of arthritis in the remaining parts of the body, arthritis is strongly considered.A Few Other Look Alikes Worth Knowing
Cervical radiculopathy and RA are the two big ones, but they aren’t alone. A short list of others that get confused with carpal tunnel:
- Wrist tendonitis – Inflammation of the tendons from overuse or repetitive motion. The giveaway is where it hurts, usually the tendon itself will be very painful, with visible swelling, and if it is caused by active movement, it will flair up, not wake you up at night.
- Ankle pain – Especially lateral, which may be caused by compression of the lateral tarsal nerve. It causes numbness in the pinky and ring fingers, quite the opposite of what is seen in carpal tunnel: the thumb-side fingers.
- Pronator teres syndrome (pinching of median nerve in the forearm, not in the wrist). There is a lot of common ground but the location of the compression is different so wrist surgery will not help.
Why the Right Diagnosis
Each of these conditions is treated differently, and cannot be passed on. The single issue that comes in with splints, steroid injections, and carpal tunnel release surgery is that the median nerve is compressed at the wrist. None of them mentions about a herniated disc in the neck or autoimmune joint inflammation.
So the simplest of all red flags is that if you are not getting better from the traditional carpal tunnel treatments, the condition itself should be re-evaluated. That’s the time to advocate for further assessment and not just going straight to surgery based on the assumption.
Generally, it can be solved with an appropriate work-up. An elaborate physical examination performed with certain maneuvers, including Spurling’s sign (extending the neck to elicit radiculopathy symptoms), electromyography or nerve conduction testing can help determine the site of the actual problem within the nerve. They are confirmed by imaging techniques such as ultrasound or MRI. This should be transported by an orthopedic specialist, neurologist or physical therapist.
But hand numbness should not be taken lightly diagnosing it correctly is even more important. The solution is only effective if it is directed towards the actual issue.
This article is for general information and isn’t a substitute for evaluation by a qualified medical professional. If the weakness, numbness or pain persists in the hands, a patient should talk to clinician about diagnosis.