
Overbite (Buck Teeth): Causes and the Best Treatment Options
An overbite is one of the most frequently diagnosed dental misalignments in the United States, ranging from a minor overlap that requires no intervention to a structural jaw discrepancy needing surgical correction. Most people use the term buck teeth interchangeably with the condition, though there is a technical distinction between the two. This article covers what causes it, what complications develop when it goes uncorrected, and which corrective options the research supports – organized by age group and severity so you can understand what applies to your situation.
Normal Overlap vs. a Bite Misalignment That Needs Attention
A small degree of vertical overlap between upper and lower front teeth is completely normal. An overlap of 2 to 4 millimeters is typical. If your upper front teeth cover more than 30% of your lower front teeth – roughly 4 to 6 millimeters – that crosses into overbite territory requiring evaluation.
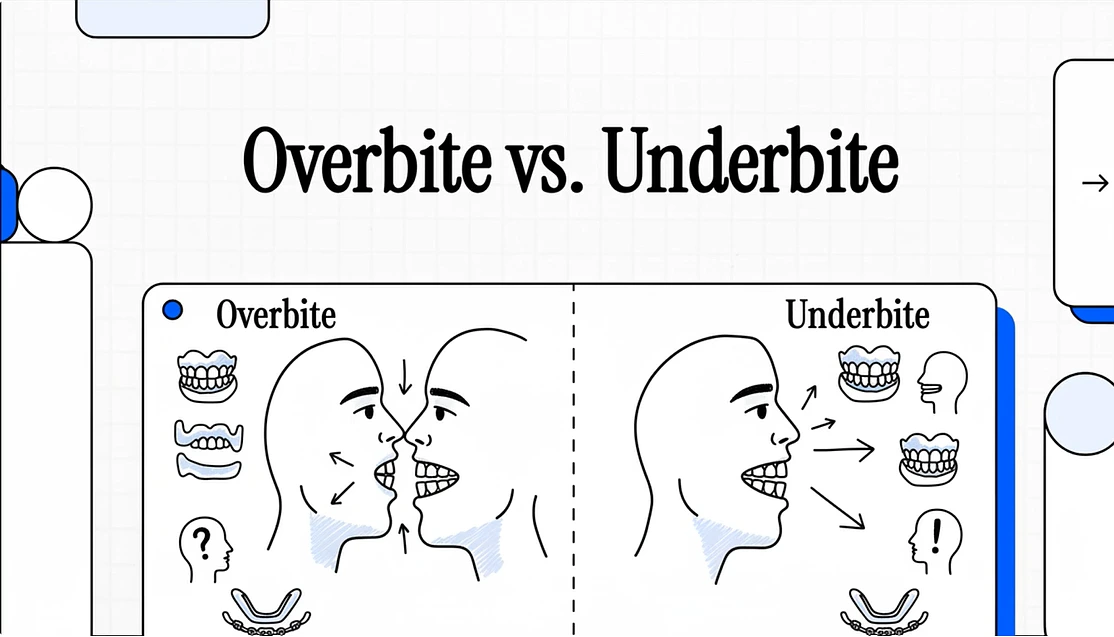
People often call protruding upper teeth buck teeth, but technically the term describes horizontal protrusion (overjet), while the vertical overlap is the actual. In practice, the two frequently occur together. An is characterized by the upper teeth significantly overlapping the lower teeth vertically, while overjet – commonly called buck teeth – refers to horizontal protrusion of the upper teeth beyond the lower teeth.
Severity is usually classified by percentage of overlap:
- Mild: Under 30% overlap, rarely causes functional problems.
- Moderate: 30 to 50% overlap, monitored closely by an orthodontist.
- Severe: Over 50% overlap, active correction typically recommended.
There are two structural categories, and the difference directly affects which corrective path is appropriate:
- Dental – caused by tooth positioning rather than the jaw structure itself. Teeth grew in at angles pushing the upper front teeth forward.
- Skeletal – caused by a structural size difference between the upper and lower jaw. This is commonly caused by a lower jaw that is too small, which positions the upper teeth further forward and causes them to cover too much of the lower teeth.
How This Misalignment Develops
Genetics
Heredity plays a significant role in jaw size and tooth positioning. If your parents or siblings have this condition, you may be genetically predisposed to developing it. The size and shape of your jaw, which are inherited traits, directly influence how teeth align. Skeletal cases are predominantly genetic. Protruding teeth that run in families usually fall into this category, which is why early intervention in children produces better outcomes than waiting until the jaw stops growing.
Childhood Habits
Prolonged thumb sucking, pacifier use beyond age three, or extended bottle feeding can alter jaw development and tooth positioning. These habits apply pressure to the developing teeth and jaw, potentially creating or worsening the misalignment over time.
Tongue thrusting – pushing the tongue against the front teeth during swallowing or speech – can also influence tooth placement during development, gradually pushing the upper front teeth forward into a protruding position.
Crowded Teeth
When the dental arch doesn’t have enough room for all adult teeth to erupt properly, some come in at angles that push the front teeth forward. This is a common contributor to dental cases in both children and adults, and one reason corrective procedures sometimes involve extractions to create space before alignment can begin.
Teeth Grinding
Teeth grinding and nail-biting can exert sustained pressure on teeth and contribute to misalignment over time. Existing protrusion can also worsen grinding, creating a cycle where both reinforce each other.
How Widespread This Condition Actually Is

A systematic review published in the International Journal of Environmental Research and Public Health (2022) – “Prevalence of Orthodontic Malocclusions in Healthy Children and Adolescents” by De Ridder, Aleksieva, Willems, Declerck, and Cadenas de Llano-Pérula, analyzing 123 studies – found a mean prevalence of Class II malocclusion (covering most presentations of this kind) of 23.8% among children and adolescents globally.
A separate global analysis titled "Global Distribution of Malocclusion Traits: A Systematic Review," published in the European Journal of Orthodontics (2019) by Lombardo et al., found that deep vertical overlap affected 21.98% of the total examined sample across permanent and mixed dentition worldwide.
What Happens When It Goes Uncorrected
A mild case rarely causes problems. A moderate to severe case that doesn’t get addressed tends to create a predictable set of complications that worsen gradually rather than stabilizing.
Accelerated Tooth Wear
An excessive overlap causes abnormal tooth wear patterns that damage enamel over time. Correcting the bite distributes biting forces more evenly across all teeth, preserving dental structure for years to come. The lower front teeth in severe cases often wear down significantly faster because they absorb impact they weren’t designed to handle.
Jaw Pain and TMJ Strain
The misaligned bite forces jaw muscles to work harder than normal to bring teeth together. This creates strain on the temporomandibular joint – the hinge connecting the jaw to the skull. A severe misalignment can put pressure on the jaw joint, create excessive strain on jaw muscles, and lead to muscle tension and pain that contributes to TMJ disorder.
It’s worth noting some nuance here. A population-based cross-sectional study of 3,033 subjects published in the Journal of Orofacial Pain (2005) – “Relationship Between Overbite/Overjet and Clicking or Crepitus of the Temporomandibular Joint” by Hirsch, John, Drangsholt, and Mancl – found that even extreme vertical overlap values were not independent risk factors for TMJ joint sounds specifically. The connection is more complex than commonly assumed, though jaw muscle fatigue from severe misalignment remains clinically recognized.
Teeth Grinding and Enamel Loss
Leaving bottom teeth exposed from a severe bite misalignment can lead to bruxism and accelerated tooth decay. The unstable resting position forces unconscious grinding or clenching, especially during sleep. When protruding teeth and bruxism occur together, the compounding enamel loss becomes harder and more expensive to address the longer it continues.
Gum Trauma
In severe cases, the lower front teeth make direct contact with soft gum tissue behind the upper front teeth every time the mouth closes. This repetitive trauma causes gum recession and bleeding, leaving the affected teeth more vulnerable to decay over time.
Speech and Chewing Difficulties
Protruding front teeth make it challenging to pronounce words with letters F, M, B, V, P, and S, and the misaligned bite means food doesn’t break down evenly during chewing.
Corrective Options Organized by Age and Severity
For Children – Ages 7 Through Early Teens
The American Association of Orthodontists recommends kids have their first orthodontic assessment by age 7. At this point, an orthodontist can spot subtle problems like an emerging bite misalignment and either monitor it or, in severe cases, intervene early.
Children’s bones are still growing and far more responsive to guidance. Early intervention takes advantage of this flexibility to achieve outcomes that become significantly harder once jaw growth stops. Approaches at this stage include:
- Palate expanders – attached to the upper molars, these widen the upper jaw during growth spurts to create proper alignment with the lower jaw.
- Headgear – worn for prescribed hours each day to correct jaw position and slow upper jaw growth relative to the lower.
- Phase 1 braces – begin guiding tooth movement before all adult teeth arrive, reducing the severity of work needed in Phase 2.
- Herbst appliance – corrects lower jaw positioning in growing patients without surgery.
- Removal of baby teeth – creates space for incoming adult teeth to erupt in better positions.
For Teens and Adults
Once the jaw stops growing, the corrective approach shifts toward moving teeth within a fixed structure rather than guiding jaw development.
Traditional Braces
The most established and versatile approach across severity levels. Brackets and wires gradually shift teeth into proper alignment, with most cases taking 18 to 24 months to complete. For skeletal cases in adults, braces are typically combined with rubber bands that apply directed force to reposition the jaw relationship. This remains the preferred path for complex cases involving significant rotation, torque, or structural correction.
Clear Aligners
Clear aligners have become a widely used alternative for teens and adults, particularly for mild to moderate presentations. A retrospective study of 50 consecutive adult patients with overlap greater than 5 mm, published in the American Journal of Orthodontics and Dentofacial Orthopedics (2021), compared Invisalign against conventional fixed appliances for severe deep bite correction. No significant differences were observed in peer assessment rating analysis or total duration between the two groups.
A systematic review published in BMC Oral Health (2019) – “A Comparison of Treatment Effectiveness Between Clear Aligner and Fixed Appliance Therapies” – found that aligner patients had a statistically significant shorter overall duration than those with braces, though braces produced superior outcomes for occlusal contact quality and torque control.
Custom trays are replaced every one to two weeks, and rubber bands may be included for bite correction, typically taking 12 to 18 months. This approach works particularly well for dental cases and mild-to-moderate buck teeth where the protrusion is positional rather than structural.
Tooth Extraction
Extraction is an option when overcrowding contributes to protrusion, involving careful removal of one or more teeth to allow the remaining teeth to shift into better alignment. It is not a standalone procedure – it creates the space needed for braces or aligners to do their work effectively.
Corrective Jaw Surgery (Orthognathic Surgery)
Reserved for skeletal cases in adults where orthodontics alone cannot produce adequate correction. In serious skeletal cases, the best approach combines oral surgery with comprehensive orthodontic care. Braces or aligners shift teeth into position first, then orthognathic surgery realigns the jaw, followed by a final round of refinement. This combined path produces stable long-term results for severe cases that would otherwise require permanent workarounds.
Retainers
A necessary final step after any corrective procedure. Retainers prevent tooth movement after correction is complete. Skipping retainer use causes relapse – teeth drift back toward their original positions, undoing months or years of work.
This article is for informational purposes only and does not constitute dental or medical advice. Consult a licensed dentist or orthodontist for diagnosis and a personalized corrective plan.
References:
- Lombardo G et al. “Global Distribution of Malocclusion Traits: A Systematic Review.” European Journal of Orthodontics. 2019. (ncbi.nlm.nih.gov/pmc/articles/PMC6340198)
- Hirsch C, John MT, Drangsholt MT, Mancl LA. “Relationship Between Overbite/Overjet and Clicking or Crepitus of the Temporomandibular Joint.” J Orofac Pain. 2005;19(3):218-25. (pubmed.ncbi.nlm.nih.gov/16106715)
- Xueru C et al. “Comparison of Clinical Outcomes Between Invisalign and Conventional Fixed Appliance Therapies in Adult Patients with Severe Deep Overbite.” American Journal of Orthodontics and Dentofacial Orthopedics. 2021. (sciencedirect.com/science/article/abs/pii/S0889540621006235)
- Ke Y, Zhu Y, Zhu M. “A Comparison of Treatment Effectiveness Between Clear Aligner and Fixed Appliance Therapies.” BMC Oral Health. 2019. (ncbi.nlm.nih.gov/pmc/articles/PMC6343314)
- Cleveland Clinic. “Overbite: Causes, Symptoms & Treatment.” (my.clevelandclinic.org/health/diseases/21473-overbite)
- Cleveland Clinic. “Overjet (Buck Teeth): What It Is and How To Fix It.” (my.clevelandclinic.org/health/diseases/overjet)