
Migraine Prevention When the Medications Stopped Working: What the Chicago Data Says About Acupuncture as the Next Step

I have been managing migraines for years now, and the medication carousel is starting to feel like a closed loop. Triptans worked at first, then started causing rebound headaches. The preventive my neurologist put me on, topiramate I think it was, dropped my migraine days a bit but the cognitive side effects were so bad I quit it. Beta blockers next. Then amitriptyline. Then the conversation about CGRP inhibitors and whether insurance would cover them. Somewhere in the middle of all that I started looking into what else might actually work, and acupuncture kept coming up in the research, not on the wellness blogs, in the actual neurology journals.
The thing I had to figure out is that the evidence for acupuncture in migraine prevention is genuinely strong, but the quality of who is delivering it varies massively, and that variation matters more in Illinois than people realize.
The Numbers Behind Why So Many Americans Hit This Wall
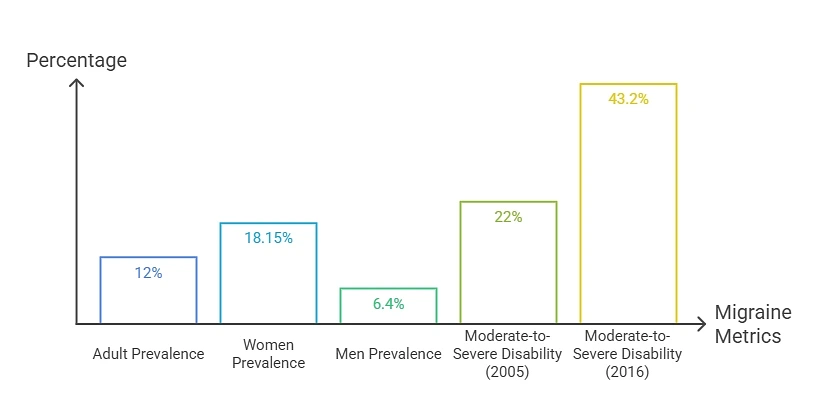
Migraine is more common in the US than most people realize. A 2024 systematic review published in Headache: The Journal of Head and Face Pain looked at 11 US population-based studies and found prevalence has stayed at roughly 12% of adults for the past three decades, with 17.1% to 19.2% in women and 5.6% to 7.2% in men. The American Migraine Foundation puts the total around 40 million Americans, with nearly 1 in 4 households including someone with the condition.
So the closed loop is well documented. Standard preventives help some people, do nothing for others, and many people end up where I am, which is somewhere between “the medications kind of work” and “the side effects are not worth it.” That is where the conversation about non-medication options starts to matter.
The Cochrane Evidence On Acupuncture For Migraine Is Stronger Than Most People Think
The single most cited piece of research on this is the 2016 Cochrane systematic review by Linde and colleagues, “Acupuncture for the prevention of episodic migraine” published in the Cochrane Database of Systematic Reviews. They pulled 22 trials covering nearly 5,000 patients and compared acupuncture against usual care, sham acupuncture, and prophylactic drugs.
The summary that made me actually take this seriously came from co-author Klaus Linde, MD, deputy director of the Centre for Complementary Medicine Research at the Technical University of Munich, when he explained the findings to Neurology Today:
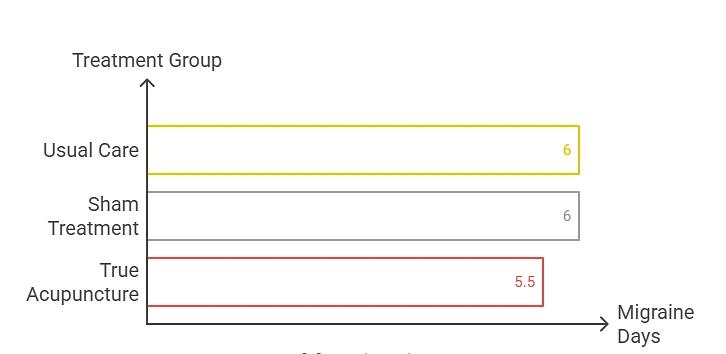
- People starting with 6 migraine days per month who received only usual care dropped to 5 days.
- People who received fake acupuncture or a prophylactic drug dropped to 4 days.
- People who received true acupuncture dropped to 3.5 days.
Headache frequency was cut in half in 50% of patients receiving true acupuncture compared to 41% receiving sham. The effect was still present at six months in the three large trials with about 1,200 people, which is the durability question most people ask first. Side effect rates between real and sham acupuncture were not significantly different and dropout rates were similar.
A 2019 systematic review in Medical Acupuncture verified the comparison against conventional drugs and concluded that for episodic migraine prophylaxis, moderate evidence suggests acupuncture is “at least non-inferior” to proven conventional treatments like flunarizine, metoprolol, and valproic acid. A 2020 Frontiers in Neurology review extended this further, finding acupuncture was at least as effective as prophylactic drugs and associated with fewer adverse effects.
Boiled down, the evidence does not say acupuncture is magic. It says acupuncture works comparably to standard preventive medications, with fewer side effects, and the effect lasts.
Why Illinois Licensing Matters More Than The Average State
Here is where the Chicago piece becomes specifically relevant. Illinois passed the Acupuncture Practice Act in January 1997, and the state’s licensing requirements are among the more rigorous in the US. The Illinois Department of Financial and Professional Regulation requires anyone practicing acupuncture in the state to meet a specific set of credentials before being allowed to put needles into anyone.
The licensing requirements include:
- Graduation from a school accredited by the Accreditation Commission for Acupuncture and Herbal Medicine (ACAHM, formerly ACAOM), which typically means a master’s-level program of three to four years.
- Passing the NCCAOM certification examination administered by the National Certification Commission for Acupuncture and Oriental Medicine, or an equivalent IDFPR-approved examination.
- Successful completion of the Clean Needle Technique course administered by the Council of Colleges of Acupuncture and Herbal Medicine.
- License renewal every two years on June 30 of odd-numbered years, with continuing education requirements documented in Title 68, Part 1140 of the Illinois Administrative Code.
The Illinois Acupuncture Practice Act defines acupuncture as “evaluation or treatment that is effected by stimulating certain body points by the insertion of pre-sterilized, single-use, disposable needles.” That definition matters because it specifically protects against unlicensed practice, and the law states that no person may treat human ailments by acupuncture in Illinois without holding a current IDFPR license.
The Illinois Chiropractic Society has clarified that the Acupuncture Practice Act also allows acupuncturists licensed by IDFPR to perform acupuncture either without a referral or pursuant to a written one, depending on the practice setting. Properly trained physicians, dentists, and chiropractors can also practice acupuncture under the Medical Practice Act, but standard of care still requires they possess adequate education and training for the technique they are performing.
What this means for anyone looking for a Chicago acupuncturist is that the state has done a real piece of the verification work for you. Anyone you see should hold a current IDFPR license, which can be verified directly through the IDFPR license lookup system. License number, expiration date, any disciplinary history, all of it is public record.
What To Look For In A Chicago Acupuncture Practice For Migraine Specifically
License verification gets you to the floor. The ceiling depends on the practice itself.
A few things worth asking before booking:
- Specific experience treating migraine and headache disorders, not just general acupuncture practice.
- Whether the practitioner uses the acupuncture point protocols that match the trials, which tend to use a combination of head and body points with electroacupuncture or manual stimulation.
- Treatment frequency and course length, with the research-supported standard being eight to twelve sessions over a few months for a fair trial of the approach.
- Integration with existing medical care, particularly whether the practitioner is comfortable communicating with your neurologist and treating acupuncture as additive to your ongoing care.
- Whether the practice operates within an integrative medicine framework that also offers chiropractic, physical therapy, dry needling, and rehabilitation, which tends to produce better outcomes for patients with overlapping musculoskeletal and headache issues.
Chicago has a well-developed integrative medicine ecosystem. Major academic medical centers like Northwestern Memorial, Rush University Medical Center, and the University of Chicago all have integrative medicine programs that include acupuncture for headache. Several established private clinics offer multi-disciplinary care models in different neighborhoods, including Lakeside Spine and Wellness Inc. in Ravenswood, which integrates acupuncture Chicago practice with chiropractic, soft tissue therapy, dry needling, and rehabilitation under one roof.
The multi-disciplinary frame matters for migraine specifically because the condition often sits alongside neck tension, jaw tension, postural patterns, and stress-related muscular issues that benefit from a broader treatment approach. A practitioner who can address the headache piece while another provider in the same practice addresses the neck and shoulder piece tends to produce better outcomes than either treatment in isolation.
What A Realistic Course Of Treatment Actually Looks Like
The expectation management problem with acupuncture is that it gets oversold by wellness marketing and undersold by people who only read one negative study. Both framings miss what the evidence actually says about typical patient response.
Based on the research and what most evidence-based practitioners describe:
- Sessions 1 to 3 – Most patients notice some change, often in sleep quality, stress baseline, or how their body holds tension. Migraine frequency does not usually drop noticeably yet, but the groundwork is being laid.
- Sessions 4 to 8 – Migraine frequency typically starts to drop, with the Cochrane data showing the average patient moving from baseline to about half the migraine days. Some patients respond faster, some slower. Patients on standard preventive medication often see the medication start working better at this point, or they discuss tapering with their neurologist.
- Sessions 9 to 12 – The course wraps up. The patients who responded well typically maintain gains with periodic maintenance sessions, monthly or every six weeks. Patients who did not respond by session twelve usually do not respond at fifteen either, which is when the practitioner should be honest about acupuncture not being the right fit and suggesting other paths.
- Six-month maintenance – The Cochrane data showed the effect was still present at six months in the large trials, which means the gains tend to hold even after the initial intensive course ends. Most patients settle into a routine of one session every month or two to maintain the improvement.
If you have been on the medication carousel for years, that timeline can feel slow. The trade-off is that you are not adding new side effects, and for patients who responded well, the long-term outcome is genuine reduction in migraine days rather than just better acute management.
What The Session Itself Is Like

The thing nobody really explains until you actually sit in the chair is that acupuncture needles are not the medical needles you are picturing. They are roughly the diameter of a thick human hair, often around 0.18 to 0.30 millimeters, compared to typical injection needles which are several times thicker. Most patients describe insertion as a mild pressure or warmth rather than a sharp sensation.
The “deqi” response, which is the physiological activation acupuncturists are aiming for, usually feels like a mild heaviness, warmth, or spreading sensation in the treated area. Some patients find it relaxing enough that they fall asleep on the table. Some find the first session strange and the second more familiar.
For migraine specifically, the needles are typically placed in a combination of points on the head, neck, hands, feet, and sometimes the legs. The session itself usually runs 30 to 60 minutes including consultation, needling, and rest time with the needles in place.
What Changes When This Works
For me, the shift was not the migraines disappearing entirely, it was the frequency dropping enough that I stopped planning my life around them. The medication conversation also changed because my neurologist was open to tapering the daily preventive once the acupuncture course showed steady gains over a few months. The acute medications still get used when a migraine breaks through, but the rebound pattern from constant triptan use eased once I was using them less often.
The honest version of this is that acupuncture is not a cure for migraine, it is a real preventive option with comparable evidence to standard medications and a different side effect profile. For anyone in Chicago who has watched the medications stop working or generate side effects worse than the condition itself, a properly licensed practitioner working in an integrative framework is a legitimate next move, supported by the same kind of randomized trial evidence the medication options are supported by.
The license verification is the first step. The right fit for the specific condition is the second. And the eight-to-twelve session window is what actually tells you whether it works for your particular case, which is the answer no article can give you in advance.