
How to Treat Multilevel Degenerative Disc Disaease
Back and neck pain are among the most common health complaints worldwide, and one of the leading causes is something called degenerative disc disease (DDD). The name sounds alarming, but DDD is not actually a “disease” in the strict medical sense it is a gradual wear-and-tear condition that develops as the spinal discs lose their flexibility, hydration, and shock-absorbing ability over time.
When this wear affects two or more discs at once, the condition is referred to as multilevel degenerative disc disease. It is more complex than single-level DDD because pain, stiffness, and nerve symptoms can occur at several points along the spine simultaneously sometimes in the neck and the lower back at the same time.
The good news? Most people with multilevel DDD can manage their symptoms successfully without surgery. With early diagnosis, the right exercises, lifestyle adjustments, and medical care when needed, you can stay active, reduce pain, and protect your spine for the long term.
What Is Degenerative Disc Disease?
Degenerative disc disease is a condition in which the soft cushions between the vertebrae of your spine known as intervertebral discs gradually break down.
Each disc has two parts:
- A tough outer ring called the annulus fibrosus.
- A soft, gel-like center called the nucleus pulposus.
These discs act like shock absorbers, allowing your spine to bend, twist, lift, and absorb impact without damaging the bones. As we age, the inner core of each disc slowly loses water, becomes less elastic, and starts to flatten. The outer ring may develop tiny cracks, and in some cases, the disc bulges or herniates, pressing on nearby nerves.
DDD is extremely common. A large systematic review published in the American Journal of Neuroradiology found that disc degeneration appears on imaging in 37% of pain-free people in their 20s and rises to 96% by age 80 (Brinjikji et al., AJNR, 2015). In other words, some level of disc wear is essentially universal as we age but it does not always cause pain. According to the Cleveland Clinic, only about 5% of adults develop chronic back pain from DDD, even though most show signs of it on scans.
Types of Degenerative Disc Disease
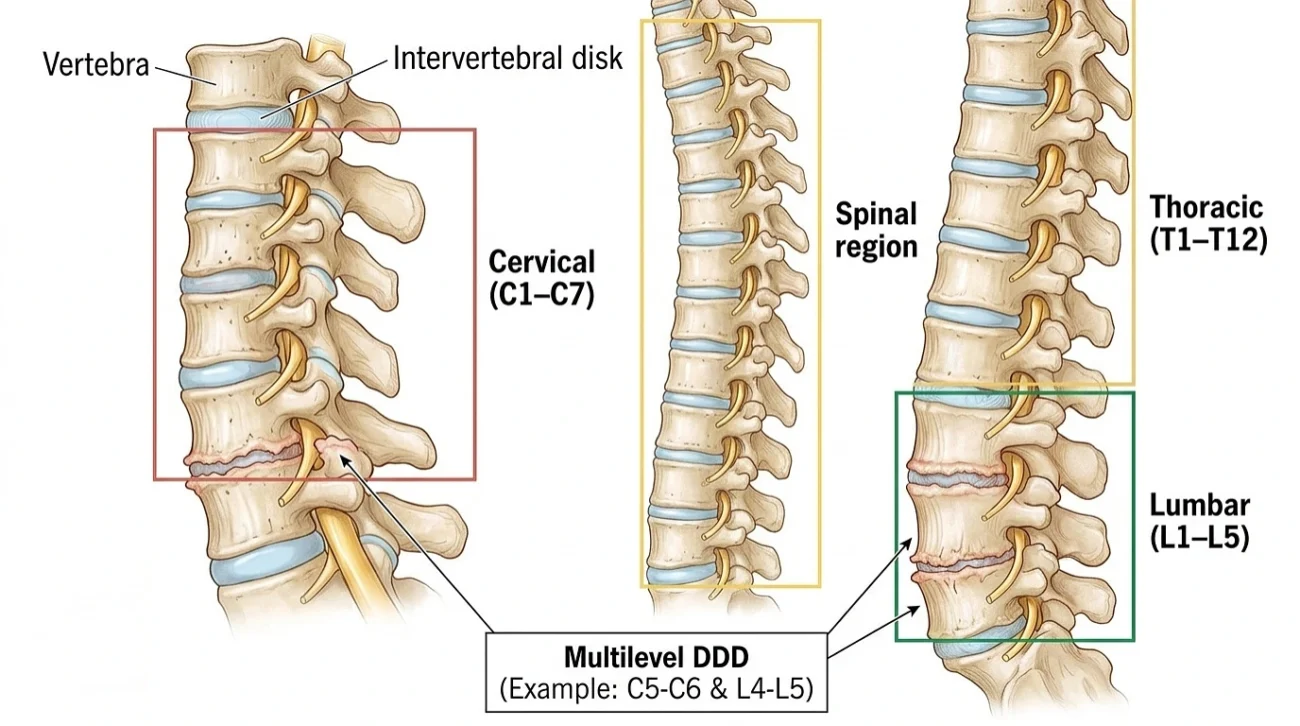
DDD is classified based on where it occurs in the spine and how widespread it is.
1. Cervical Degenerative Disc Disease
This affects the seven vertebrae of the neck (C1–C7). Common symptoms include neck stiffness, headaches, and pain or tingling radiating into the shoulders, arms, or hands. Because cervical discs support the weight of the head and allow significant motion, they are highly prone to wear.
2. Thoracic Degenerative Disc Disease
This affects the mid-back (T1–T12). It is the least common form because the thoracic spine is naturally more rigid and protected by the rib cage. When symptoms do appear, they include mid-back pain, chest discomfort, or pain wrapping around the torso.
3. Lumbar Degenerative Disc Disease
The most common form, affecting the lower back (L1–L5). Lumbar discs bear the most body weight and absorb the greatest impact during walking, lifting, and bending. Symptoms include chronic lower back pain, stiffness, and sciatica pain radiating through the buttocks and down one or both legs.
4. Multilevel Degenerative Disc Disease
This is when two or more discs show degeneration at the same time. It may occur entirely within one region (such as multiple lumbar levels) or across two regions simultaneously for example, both cervical and lumbar levels. A study based on the long-running Framingham research project, published in The Spine Journal, reported that one-third of people aged 40 to 59 already have moderate-to-severe degenerative disc disease on imaging (Samelson et al., The Spine Journal, 2018). Multilevel DDD is generally more complex than single-level DDD because each affected level can produce its own symptoms and respond differently to treatment.
Symptoms and Causes of Degenerative Disc Disease
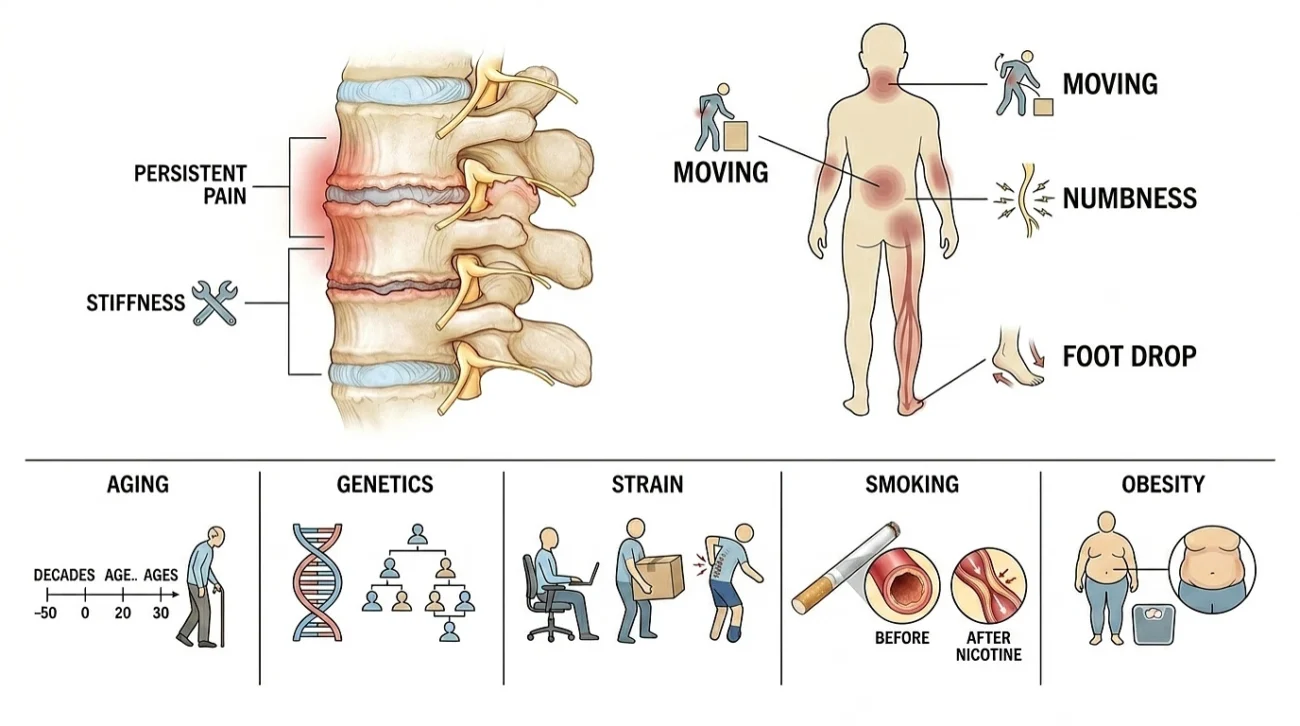
Common Symptoms
Symptoms of DDD vary widely from person to person. Some people have severe pain, while others have noticeable disc damage on MRI but feel almost nothing. Typical signs include:
- Persistent neck or lower back pain that comes and goes in flare-ups.
- Pain that worsens with sitting, bending, lifting, or twisting.
- Stiffness, especially in the morning or after long periods of inactivity.
- Pain that radiates into the arms, shoulders, buttocks, thighs, or legs.
- Numbness, tingling, or weakness when nerves are pinched.
- Reduced flexibility and range of motion.
- Muscle spasms in the neck or back.
- Pain that improves when lying down or changing positions.
In severe cases, compressed nerves can cause leg weakness, foot drop, or in rare emergencies loss of bladder or bowel control. These signs require immediate medical attention.
Common Causes and Risk Factors
While aging is the leading cause of DDD, several other factors can speed up the process:
- Aging – Disc dehydration starts in the 20s and progresses with each decade.
- Genetics – A family history of spine problems significantly raises your risk.
- Repetitive strain – Heavy lifting, prolonged sitting, or jobs involving frequent twisting and bending.
- Acute injuries – Falls, sports injuries, or car accidents that damage disc structure.
- Smoking – Research published in PLOS One showed that nicotine constricts the blood vessels surrounding the disc and reduces nutrient supply, contributing directly to disc breakdown (Vergroesen et al., PLOS One, 2015). An earlier laboratory study in Spine also confirmed that nicotine reduces the proliferation and survival of disc cells (Akmal et al., Spine, 2004).
- Obesity – Excess weight, especially around the midsection, multiplies pressure on the lumbar spine.
- Sedentary lifestyle – Weak core and back muscles leave the spine unsupported.
- Poor posture – Constant slouching, screen time, and forward-head posture accelerate cervical wear.
Understanding your personal risk factors is the first step toward slowing progression many of them are within your control.
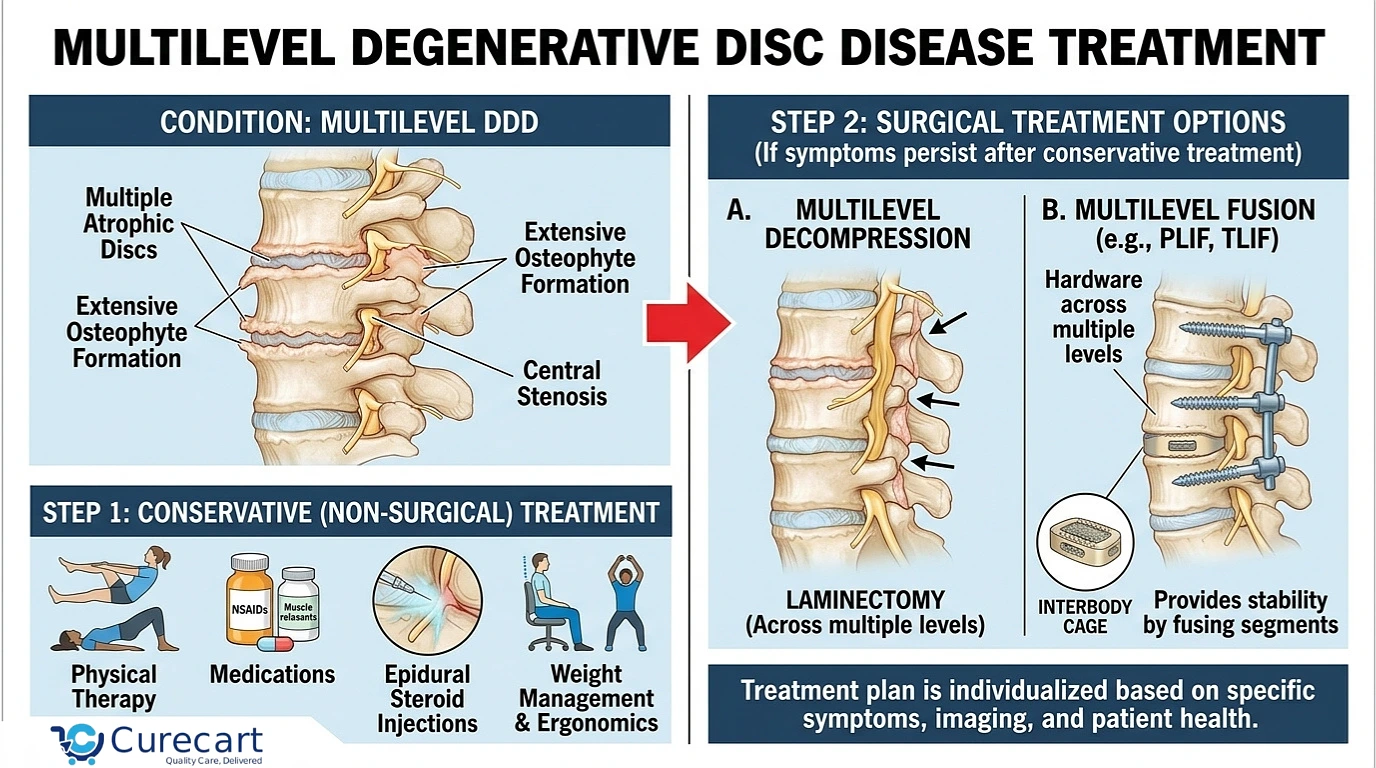
Multilevel Degenerative Disc Disease Treatment
Treating multilevel DDD almost always follows a step-by-step approach: start with the least invasive options and escalate only when symptoms persist. Current international guidelines, including those summarized by the American Physical Therapy Association and the North American Spine Society (NASS), recommend conservative management as first-line care for the vast majority of cases.
Conservative Treatment (First Line of Care)
Most cases respond well to non-surgical care over a 6 to 12 week period. The goal at this stage is to reduce pain, restore mobility, and strengthen the muscles that support the spine.
Physical Therapy
Physical therapy is the cornerstone of treatment. A trained physiotherapist will design a program tailored to your specific affected levels. Common components include:
- Core strengthening – bridges, bird-dogs, dead bugs, and planks to build the deep abdominal and back muscles that stabilize the spine.
- Flexibility work – cat-cow stretches, hamstring stretches, and gentle spine mobility drills.
- Posture correction – retraining how you sit, stand, and lift.
- McKenzie extensions – particularly helpful for lumbar DDD with mild bulging.
- Manual therapy – hands-on techniques to relieve muscle tension and improve joint movement.
Medications
Pain relief medications help patients stay active enough to benefit from physical therapy. Common options include:
- NSAIDs such as ibuprofen or naproxen for inflammation.
- Acetaminophen (paracetamol) for general pain relief.
- Muscle relaxants for short-term spasm control.
- Nerve-pain medications like gabapentin or pregabalin when nerves are involved.
Always use medications under medical supervision long-term NSAID use can cause kidney and stomach problems.
Lifestyle Modifications
This is where patients have the most long-term control:
- Quit smoking – directly slows disc breakdown by improving blood flow to spinal tissues.
- Maintain a healthy weight to reduce spinal load.
- Stay active daily – walking, swimming, and cycling are ideal low-impact options.
- Improve posture and ergonomics – adjust your workstation, use a supportive chair, and avoid prolonged sitting.
- Manage stress, which amplifies pain perception.
- Sleep smart – use a medium-firm mattress and side-sleep with a pillow between the knees.
Step 2: Interventional Pain Management
If conservative care does not provide enough relief, minimally invasive procedures can help without crossing into surgery. These are usually performed by a pain management specialist.
- Epidural steroid injections – deliver anti-inflammatory medication directly to the affected nerve roots, offering weeks to months of relief.
- Facet joint injections – target the small joints between vertebrae that often become painful in multilevel DDD.
- Radiofrequency ablation (RFA) – uses controlled heat to disable the small nerves carrying pain signals, often providing 6 to 12 months of relief.
- Spinal cord stimulation (SCS) – an implanted device that sends mild electrical signals to interrupt pain pathways before they reach the brain.
Step 3: Surgical Treatment (Last Resort)
Surgery is considered only when:
- Conservative and interventional treatments have failed after several months.
- There is significant nerve compression causing weakness or numbness.
- Quality of life is severely impacted.
- Imaging shows clear structural problems that surgery can correct.
For the lumbar spine:
- Spinal fusion (TLIF, LLIF, ALIF) – joins two or more vertebrae together to eliminate painful motion.
- Artificial disc replacement – preserves spinal motion in select candidates.
For the cervical spine:
- Anterior Cervical Discectomy and Fusion (ACDF) – the long-standing standard for multilevel cervical DDD.
- Cervical Disc Replacement (CDR) – a newer motion-preserving option. A meta-analysis published in Medicine found that multilevel CDR was associated with lower rates of adjacent segment degeneration and fewer adverse events compared with multilevel ACDF, though the authors noted that longer-term studies are still needed (Zhao et al., Medicine, 2017).
Multilevel surgery is more complex than single-level procedures and requires longer recovery, so it is reserved for cases where the benefits clearly outweigh the risks.
FAQs
Is multilevel degenerative disc disease a serious condition?
It is usually manageable, but becomes serious if nerve compression causes weakness, numbness, or loss of bladder control.
Can multilevel degenerative disc disease be cured?
No, but symptoms can be controlled. Treatment slows progression and keeps you active and pain-free.
Is multilevel DDD considered a disability?
It can be, if it severely limits your ability to work or move and imaging confirms significant degeneration.
Can I live a normal life with multilevel degenerative disc disease?
Yes. With early treatment, daily movement, and good posture, most people continue a fully active life.
Is walking good for degenerative disc disease?
Yes, it is one of the best exercises. A 20 to 30 minute daily walk improves blood flow and reduces stiffness.
When should I see a doctor about my back or neck pain?
See a doctor if pain lasts more than a few weeks or comes with numbness, tingling, or weakness in your limbs.
References
- Brinjikji W, et al. Systematic Literature Review of Imaging Features of Spinal Degeneration in Asymptomatic Populations. American Journal of Neuroradiology (AJNR), 2015. https://pmc.ncbi.nlm.nih.gov/articles/PMC4464797/
- Cleveland Clinic. Degenerative Disk Disease: Symptoms, Causes & Treatment. https://my.clevelandclinic.org/health/diseases/16912-degenerative-disk-disease
- Samelson EJ, et al. A longitudinal study of disc height narrowing and facet joint osteoarthritis of the spine in the Framingham Study. The Spine Journal, 2018. https://www.sciencedaily.com/releases/2018/05/180517163317.htm
- Vergroesen PA, et al. Effects of Tobacco Smoking on the Degeneration of the Intervertebral Disc: A Finite Element Study. PLOS One, 2015. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0136137
- Akmal M, et al. Effect of nicotine on spinal disc cells: a cellular mechanism for disc degeneration. Spine, 2004.
- Zhao Y, et al. Multilevel cervical disc replacement versus multilevel anterior discectomy and fusion: A meta-analysis. Medicine, 2017.
- American Physical Therapy Association (ChoosePT). Physical Therapy Guide to Degenerative Disk Disease.
- North American Spine Society (NASS). Clinical Practice Guidelines.