Recognising the Early Signs of Dissociative Identity Disorder: What the Symptoms Actually Look Like
Key Takeaway
Dissociative identity disorder is rarely recognised by its most famous feature. The early signs are quiet lost time, accounts of yourself you cannot remember, a persistent sense of detachment and they are easy to explain away for years. The symptom that matters most is not “different personalities” but dissociative amnesia: genuine, repeated gaps in the memory of your own life. Because the condition closely resembles several others and affects memory itself, recognising the signs is a reason to seek assessment, never a substitute for it.
You lose time. Not the ordinary kind, where an afternoon slips by because you were absorbed in something. The kind where you arrive somewhere and cannot account for the last two hours. Where someone insists you had a conversation you have no memory of. Where you find clothes in your wardrobe, or messages on your phone, that you do not remember buying or sending.
For most people this never happens. For someone living with dissociative identity disorder, it can be the texture of an ordinary week and it is often years before anyone names what is going on.
DID is one of the least understood disorders in mental health. It’s not something that’s usually the obvious, grand thing that films would have you think. Early symptoms are more subtle, can be dismissed and are often confused for something else. That is the reason that people do not recognise the condition for so long, that which they see and the expected image of the condition.
What Dissociative Identity Disorder Actually Is
Dissociative identity disorder is a condition in which a person’s sense of self is split across two or more distinct identity states, alongside gaps in memory that go beyond ordinary forgetting. It was previously called multiple personality disorder, a name that has been retired because it framed the condition as “extra people” rather than what it actually is: a fragmentation of one identity that never fully integrated in the first place.
The current diagnostic standard, the DSM-5-TR, describes it as a disruption of identity marked by two or more distinct personality states, with recurrent gaps in recall of everyday events, personal information, or traumatic events that are inconsistent with normal forgetting.
The mechanism most clinicians work from is developmental. Severe, repeated trauma in early childhood typically before the age of six to nine, when identity is still forming can interrupt the normal process by which a child consolidates a single, continuous sense of self. Instead of one integrated identity, separate states develop, each holding different memories, behaviours, and ways of coping. Dissociation, in this view, is not a malfunction. It begins as a survival strategy for a child who has no other escape.
Why It Is So Often Missed
Here is the part that matters for early recognition: people with DID rarely walk into a clinic and report having multiple identities. That is almost never the presenting complaint.
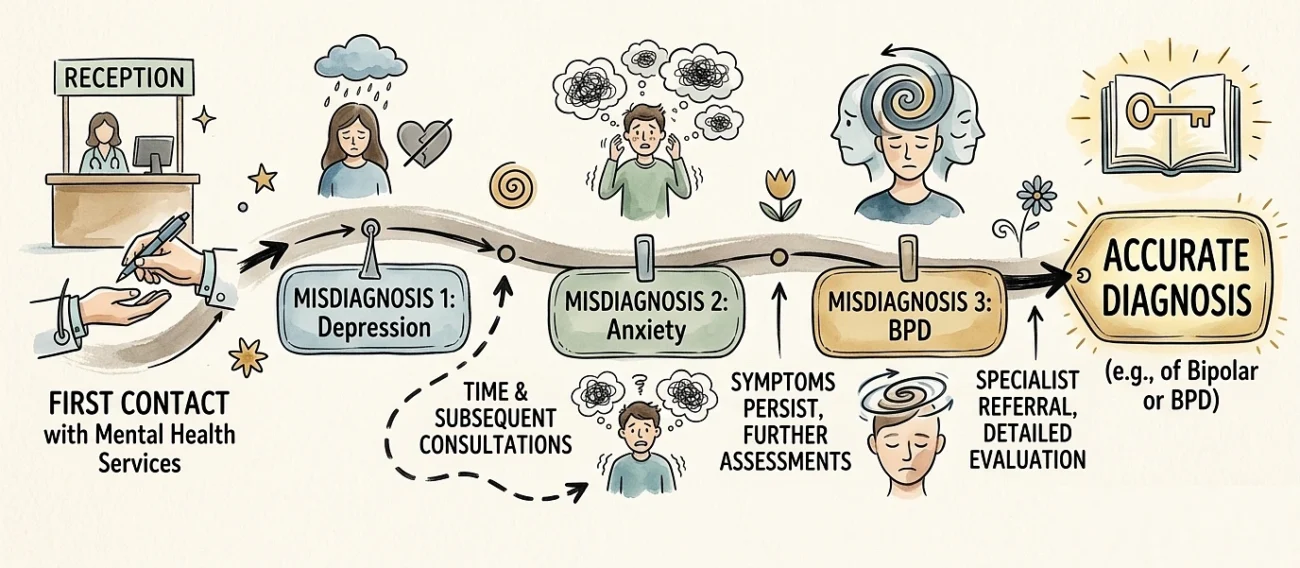
Research on diagnosis has repeatedly found long delays between first contact with mental health services and an accurate diagnosis often several years, sometimes a decade or more with patients frequently receiving other diagnoses first. There are concrete reasons for this.
The person themselves often cannot see it. The defining feature of the condition amnesia between states means the part of the person sitting in the clinic may have no memory of the experiences that would point to the diagnosis. You cannot report what you do not remember.
The visible symptoms point elsewhere. What brings people in is usually depression, anxiety, self-harm, mood swings, insomnia, or unexplained physical complaints. These get treated on their own terms, and the underlying pattern is never connected.
It is heavily masked. Many people with DID spend enormous energy appearing normal covering for memory gaps, explaining away lost time, avoiding situations where the gaps would show. This masking is so effective that close family sometimes never suspect it.
The Early Signs That Are Easy to Explain Away
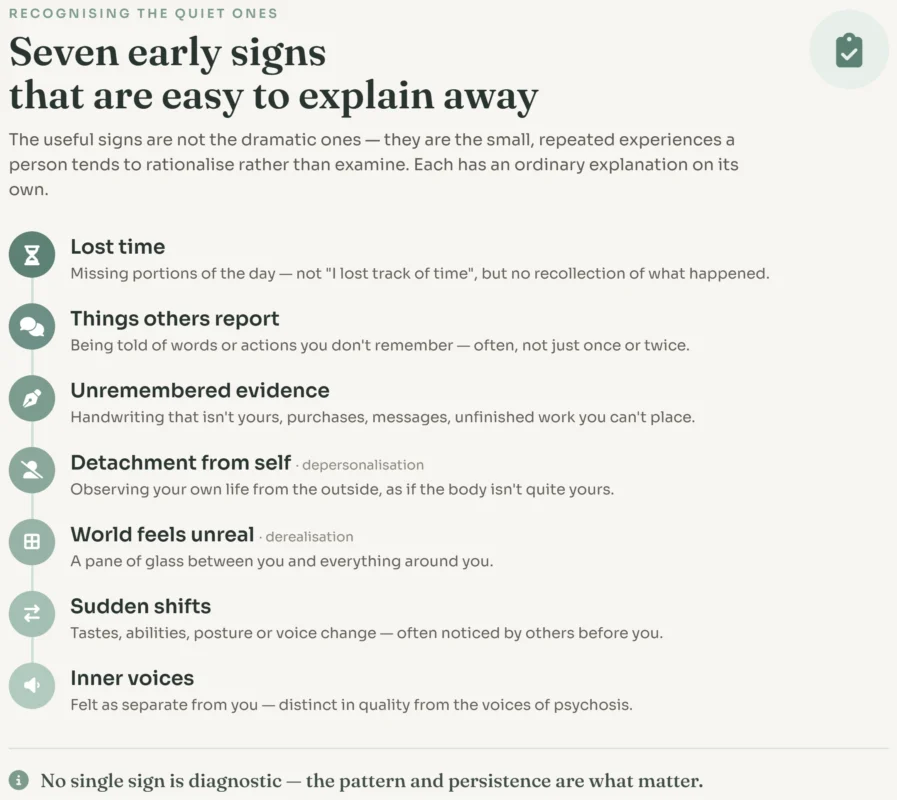
The genuinely useful signs are not the dramatic ones. They are the small, repeated experiences that a person tends to rationalise rather than examine. Taken alone, each has ordinary explanations. It is the pattern and persistence that matters.
A single one of these, occasionally, is not a diagnosis of anything. Most people dissociate mildly at times highway hypnosis, zoning out, getting lost in a task. The line worth paying attention to is when these experiences are frequent, when they cause real disruption, and when memory gaps are involved.
The Core Symptom Most People Get Wrong
If there is one thing to take from this article, it is this: the central feature of DID is not “switching between personalities.” It is dissociative amnesia the loss of memory between states.
Popular portrayals fixate on the visible switch: the change in voice, the different name, the dramatic transformation. In reality, the switches are often subtle and the amnesia is the engine of the whole condition. Someone can have DID and never present an obvious, theatrical change of personality in front of others. What they cannot avoid is the memory loss the gaps that do not add up, the missing hours, the accounts of their own behaviour they cannot verify from the inside.
That is why people are misled when they ask themselves “Do I have different personalities?”. The more important question is this: Do I have any obvious and recurring memory gaps that do not seem to be normal forgetfulness or lapses in my own life? Of all the symptoms, that one is the most distinguishing.
What the Diagnostic Criteria Actually Require
The DSM-5-TR sets out five criteria, all of which must be met. However, they are valuable to understand exactly, as they illustrate just how high the bar is and why it’s not possible to self-diagnose.
- Two or more identity states that involve a significant change in sense of self and agency with associated changes in affect, behaviour, memory, perception and functioning.
- Frequent failures of memory for routine and significant personal information, or for traumatic events which are not congruent with forgetting.
- The symptoms result in clinically significant distress or impairment in social, occupational, or other important areas of functioning.
- The disturbance is not part of a broad accepted cultural or religious practice. (This criterion exists specifically because some normal cultural and spiritual experiences can resemble dissociation but are not disorders.)
- The symptoms are not attributable to substances such as alcohol-related blackouts or another medical condition such as complex partial seizures.
That fourth and fifth criterion are where careful diagnosis lives. A great deal of what looks like dissociation has another explanation, and ruling those out is a clinician’s job, not a checklist’s.
How Clinicians Tell DID Apart From Other Conditions
Accurate diagnosis is largely a process of distinguishing DID from conditions it resembles. This is the part no symptom list on the internet can do for you, and the reason professional assessment matters.
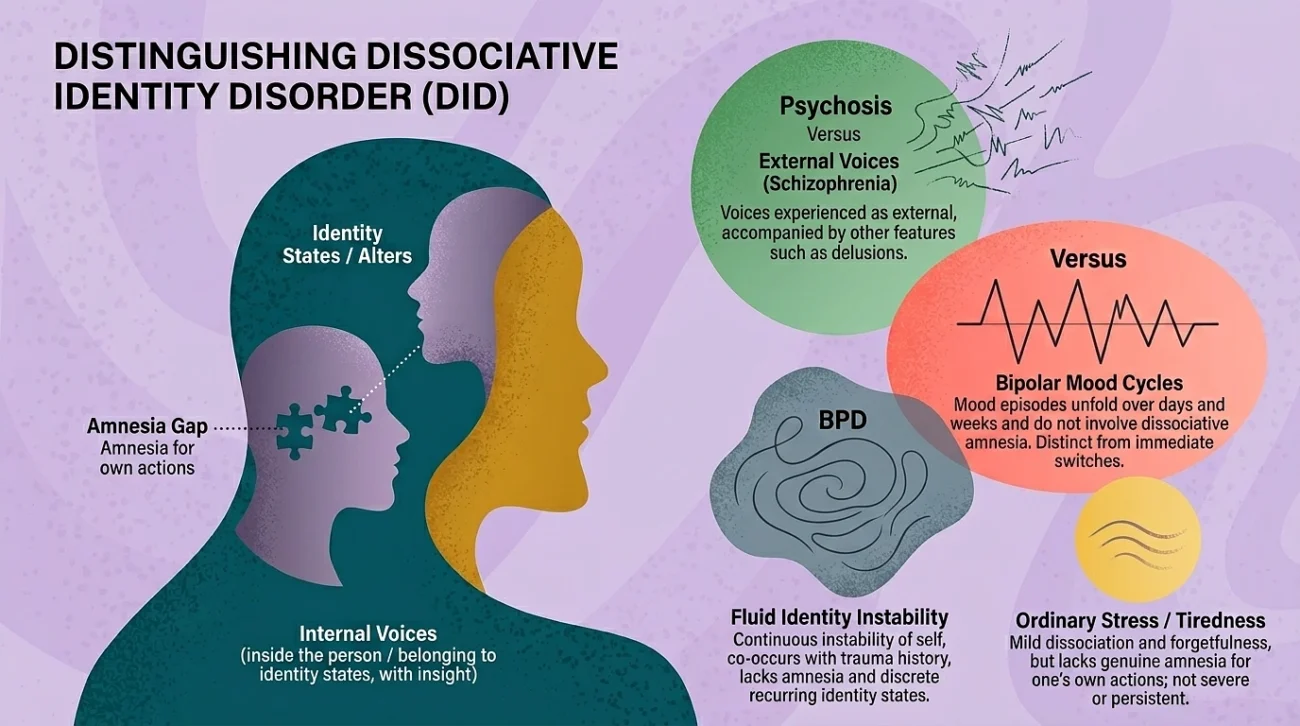
- Versus psychosis (schizophrenia). The internal voices in DID are usually experienced as coming from inside the person and as belonging to identity states, with the person retaining insight. In schizophrenia, voices are more often experienced as external and are accompanied by other features such as delusions. The two are genuinely confused in practice, and misdiagnosis in this direction is common.
- Versus borderline personality disorder. Both involve identity disturbance and a trauma history, and the two frequently co-occur, which complicates things further. The distinguishing feature is the amnesia and the presence of discrete, recurring identity states in DID, rather than the more fluid, continuous instability of self seen in BPD.
- Versus bipolar disorder. The “mood swings” of DID are switches between states that can happen within minutes and are tied to memory gaps. Bipolar mood episodes unfold over days and weeks and do not involve dissociative amnesia.
- Versus ordinary stress and tiredness. Sleep deprivation, extreme stress, and burnout all produce mild dissociation and forgetfulness. The difference is severity, persistence, and whether genuine amnesia for one’s own actions is present.
Doctors don’t just go by appearances. There are structured tools for this diagnosis because it is so easily misdiagnosed: DES as a screening tool and formal assessment by structured clinical interviews like the SCID-D. They are not self-tests and are given and interpreted by trained professionals.
What Self-Recognition Can and Cannot Do
It is worth being direct about the limits of an article like this. Recognising possible signs in yourself is valuable for one reason only it can move you toward a proper assessment sooner. That is the whole purpose of early recognition.
What it cannot do is give you a diagnosis. DID sits at the intersection of several diseases & conditions that look alike, it has criteria that require professional judgement to apply, and by its own nature it affects the very memory you would need to assess yourself accurately. Self-diagnosis here is unusually unreliable, more so than for most conditions.
There is also a specific modern pressure worth naming. Dissociation and DID have become heavily discussed on social media, and a great deal of that content is inaccurate or dramatised. Recognising your experience in a video is not the same as having a condition, and the conditions that do explain dissociative experiences are wide-ranging. The honest move, if these signs feel familiar, is not to settle on an answer yourself but to take what you have noticed to someone qualified to sort through it.
When to Consult a Specialist
Consider speaking to a psychiatrist or clinical psychologist if you notice a persistent pattern of the following, rather than isolated incidents:
- Repeated, unexplained gaps in your memory of everyday events
- Being regularly told about your own behaviour that you cannot recall
- Frequent episodes of feeling detached from yourself or your surroundings
- Distress or disruption to work, relationships, or daily life as a result
If these experiences are linked to being self-destructive, suicidal or if they are the result of a trauma in the past that is not resolved, seek help sooner rather than later. A clinician is able to determine whether dissociation is occurring, differentiate it from other conditions that can mimic it, and figure out what is really going on the first step toward any treatment that can help.
If you are in immediate distress or thinking about harming yourself, this is a sensitive area, and reaching a mental health professional or a crisis line in your area should come before anything else.
Disclaimer: The content of this article is meant to bring awareness to a complicated mental health disorder and should not be used as a diagnostic instrument or replacement for professional medical advice. It can only be diagnosed by a mental health professional. If you, or someone you know, experience similar things as described here, make sure that you consult a psychiatrist or clinical psychologist for an appropriate assessment.
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). American Psychiatric Publishing, 2022.
- Reinders, A.A.T.S., & Veltman, D.J. “Dissociative identity disorder: out of the shadows at last?” The British Journal of Psychiatry, Vol. 219, Issue 2, 2021, pp. 413–414.
- Brand, B.L., et al. “Separating Fact from Fiction: An Empirical Examination of Six Myths About Dissociative Identity Disorder.” Harvard Review of Psychiatry, Vol. 24, Issue 4, 2016, pp. 257–270.
- Spiegel, D., et al. “Dissociative disorders in DSM-5.” Depression and Anxiety, Vol. 28, Issue 9, 2011, pp. 824–852.