
Flat Affect: Causes, Associated Conditions and Treatment Options
Key Takeaway
With a flat affect individual, be mindful of this: Flat affect does not imply no affect. That calm expression could actually be a mask of uncontrollable happiness, overwhelming sadness or crushing anxiety they simply can’t reveal to you.
Talk to mental health professionals with experience in your underlying condition:
- In schizophrenia: Look for clinicians who have experience with CBT for negative symptoms and psychosis.
- For Parkinson’s: Collaborate with movement experts who are familiar with motor and emotional symptoms.
- With regards to TBI: Search for rehab that treats cognitive and emotional symptoms as a whole.
- In the case of depression: Talk to your psychiatrist about the side-effects of the medications – there are other options.
- For autism: Talk to therapists who know that differences are not deficits.
And for everyone else: practice interpreting emotional content from words and context rather than relying solely on facial cues. Some people’s emotional lives run just as deep as yours – they just express differently.
Flat affect isn’t about lacking emotions. It’s about the complete disconnect between what someone’s feeling inside and what shows up on their face, in their voice, or through their body language. And that gap? It creates problems most of us never consider.
What Flat Affect Actually Looks Like
Picture this. You have great news to share with a friend. Their voice is flat, their face doesn’t move, and their body hardly changes. You would likely leave them confused and perhaps injured. But what if they were really excited for you, and maybe they were really happy, and maybe their brain couldn’t translate that happiness?
It shows up as a severe reduction in emotional expressiveness. The key signs include:
- Monotone voice with no inflection – think of that automated GPS voice, except it’s coming from a human.
- Neutral facial expressions that don’t change even during events that would normally trigger visible reactions.
- Minimal or absent gestures and body language shifts.
- Lack of eye contact or blank stares during conversations.
- No visible emotional response to joy, sadness, anger, or fear.
The Brain Mechanisms Behind the Mask
When you experience an emotion, several brain regions fire up simultaneously:
- The limbic system processes the feeling itself.
- The prefrontal cortex helps you evaluate and regulate that emotion.
- Motor areas coordinate the physical expression – facial muscles contract, vocal cords adjust pitch, posture shifts.
Schizophrenic patients are shown to have reduced limbic structure activity in response to emotional stimuli. Blunted responses of the amygdala (normally a “Christmas tree” during emotional processing).
In Parkinson’s disease, it’s different. The “masked face” happens because dopamine depletion affects motor control. These folks feel emotions just fine – their facial muscles just won’t cooperate. Studies published in the journal Brain documented how Parkinson’s patients show muted physiological reactivity to emotional stimuli, suggesting both motor and deeper emotional processing changes.
Traumatic brain injury creates yet another pattern. When the prefrontal cortex gets damaged from a hard hit, the injury disrupts connections between feeling centers and expression centers. The emotion exists, the pathways to display it don’t function properly.
Schizophrenia: Where Flat Affect Gets Most Attention
Ask mental health professionals, and schizophrenia comes up first. There’s good reason.
Flat affect ranks as one of the most prominent negative symptoms in schizophrenia – those things that are absent when they should be present. While positive symptoms like hallucinations grab headlines, negative symptoms including actually predict long-term outcomes better.
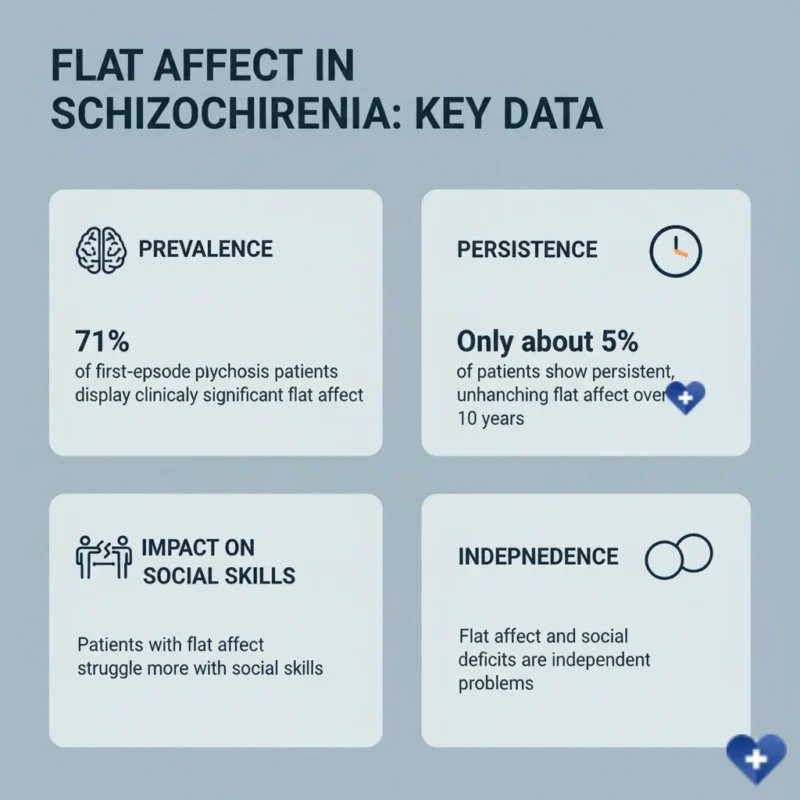
The Positive and Negative Syndrome Scale, better known as PANSS among clinicians. This standardized measurement tool, developed in 1987 by Kay, Fiszbein, and Opler for the journal Schizophrenia Bulletin, remains the gold standard for evaluating schizophrenia symptoms today.
Here’s what research shows: approximately 71% of first-episode psychosis patients display clinically significant at some point during a 10-year follow-up period, based on studies tracking PANSS scores over time. But here’s the surprising part – only about 5% show persistent, unchanging throughout that entire decade.
The discrimination matters because treatment approaches differ.
Parkinson’s Disease: When Muscles Won’t Match Mood
About 40-50% of Parkinson’s patients experience depression, and sorting out true depression from Parkinson’s motor symptoms creates diagnostic headaches. That “masked face” or hypomimia – reduced facial expression – looks identical to depression on the surface.
But the mechanisms diverge completely. Research examining emotional reactivity in Parkinson’s patients found something fascinating: these individuals show blunted startle responses to both positive and negative emotional stimuli. Scientists describe this as a “bradylimbic” disturbance – essentially, emotional processing slows down just like movement does.
The dopamine link is a long one. As dopamine-producing cells of the substantia nigra deteriorate, it impacts more than just movement. Dopamine and emotional processing pathways overlap. A research following the changes of the facial expression on phonation tests in patients with Parkinson’s disease have shown:
- Decreased expressions of happiness, surprise, and arousal.
- Increased displays of sadness, anger, and fear.
- Progressive worsening that correlates with disease severity.
Depression and the Emotional Numbness Problem

The distinction gets murky. Emotional blunting means not feeling emotions strongly – you’re actually numb inside. Flat affect means feeling emotions but not expressing them. In depression, you often get both happening simultaneously.
Here’s where medication complicates things further. SSRIs – those antidepressants like Prozac, Zoloft, and Paxil that millions take daily – can cause emotional blunting as a side effect. One study found that nearly 75% of people in the acute phase of depression reported severe emotional blunting, and about 45% blamed their antidepressants for negative effects on their emotions.
That creates a treatment dilemma. Stop the medication that’s preventing suicidal thoughts because it’s also preventing joy? The balance gets tricky.
Traumatic Brain Injury: When Impact Steals Expression
TBI affects over 2 million Americans annually through emergency department visits, hospitalizations, and deaths. The injury itself happens in two stages: primary damage from the initial impact, and secondary injury that develops over hours to years afterward.
The damage typically involves frontal lobe and limbic system structures. When these areas sustain injury, the person retains emotional experience but loses the ability to coordinate its expression.
- Cognitive difficulties including memory problems and concentration issues.
- Persistent headaches and migraines.
- Sensitivity to light and sound.
- Sleep disturbances and fatigue.
- Mood changes including depression and irritability.
The whole package creates a syndrome that’s tough to treat with isolated interventions.
Research on TBI treatment remains frustratingly limited. While we’ve made massive strides understanding the injury mechanisms, we haven’t translated that knowledge into effective therapies.
Autism Spectrum Disorder and Facial Expression Differences

The challenge is not emotional processing itself, but often reading and making facial expressions. People with autism have the same emotions as others. They may not intuitively know how to match their internal state to the facial expression, or they may not intuitively express facial images.
This isn’t a deficit requiring fixing – it’s a difference in how the brain processes social communication. The emotion exists, the social signaling works differently.
Treatment: Addressing Root Causes
In the case of schizophrenia, it’s a base of antipsychotic drugs. The interesting part of research is this: Traditional antipsychotics are very effective for the positive symptoms (such as hallucinations and delusions).
Cognitive behavioral therapy shows more promise for negative symptoms. Studies examining CBT specifically designed for negative symptoms – shortened to CBT-n in research literature – found moderate improvements. One pilot study reported an effect size of 1.26 on negative symptoms after an average of 17.5 sessions.
But the results are mixed. The TONES Study was a large randomized trial that compared CBT to cognitive remediation for the treatment of negative symptoms of schizophrenia. Result? There was a moderate gain for both groups with no significant difference between the treatments. The bottom line: psychotherapeutic intervention is beneficial; however, we cannot say that CBT provides any specific benefit over any other structured intervention.
Treatment approaches by condition:
- For Parkinson’s patients: Dopaminergic medications like levodopa help motor symptoms including facial rigidity. Physical therapy and speech therapy can specifically target facial expression and prosody – the musical quality of speech.
- For depression-related cases: Switching antidepressants sometimes helps. Newer medications like vortioxetine may produce less emotional blunting than traditional SSRIs, though individual responses vary wildly.
- For TBI rehabilitation: A multifaceted approach including cognitive therapy, physical therapy, occupational therapy, and speech-language pathology.
What About Medication Side Effects?
This deserves its own section because it’s common and reversible.
Antipsychotic medications, particularly first-generation ones, can cause flat affect as a side effect. The mechanism involves dopamine blockade affecting both motor and emotional processing circuits. Second-generation antipsychotics produce this less frequently but it still happens.
SSRIs cause emotional blunting in significant numbers of users. Estimates vary, but somewhere between 40-60% of people taking SSRIs report some degree of emotional numbness or blunted affect.
The potential fixes include:
- Switching to a different medication in the same class.
- Lowering the dose if symptoms allow.
- Adding or switching to medications with different mechanisms (like vortioxetine for depression).
- Weighing reduced symptoms against reduced emotional range – sometimes you’re stuck making that choice.
The Social Cost Nobody Calculates
Here’s what the research papers don’t emphasize enough.
People interpret lack of expression as lack of caring. The real-world consequences stack up:
- Job interviews go poorly because the candidate seems disinterested or unmotivated.
- Friendships fade because the person appears emotionally unavailable or indifferent.
- Family members feel rejected by blank faces that actually accompany deep love.
- Romantic relationships struggle when partners can’t read emotional cues.
- Social isolation increases as others pull away from perceived coldness.
The misinterpretation creates a feedback loop. Others pull away, which increases isolation, which worsens mental health. Breaking that cycle requires education – helping people understand that emotional expression and emotional experience aren’t the same thing.
Measuring and Monitoring Progress
Clinicians use several assessment tools beyond PANSS:
- The Scale for Assessment of Negative Symptoms (SANS) includes a blunted affect subscale.
- The Brief Negative Symptom Scale (BNSS) offers more refined measurement of diminished emotional expression.
- The Clinical Assessment Interview for Negative Symptoms provides structured evaluation.
- The Motor-Affective-Social Scale (MASS) captures multiple dimensions of negative symptoms.
These scales rely on trained observers rating expression during interviews. They’re subjective but standardized. Researchers are exploring more objective measures – computerized analysis of facial micro-expressions, voice prosody analysis, body movement tracking. These technologies might eventually offer quantitative biomarkers for treatment response.
Looking Forward: What Research Promises
Several promising directions exist:
- There are initial indications that NF training can assist patients with TBI in enhancing frontal lobe activity associated with emotional expression.
- Social cognition training for schizophrenia encompasses training on both emotion recognition and emotion expression.
- Mobile-assisted cognitive behavioral therapy (CBT) is a blend of in-person therapy and smartphone apps designed for daily practice.
- The development of drugs is ongoing targeting the negative symptoms specifically: using compounds that affect different neurochemical systems.
- New, sophisticated brain imaging tools are used to determine which brain circuits require intervention.
The fundamental challenge remains: we’re trying to reconnect experience and expression when the wiring between them has been damaged or disrupted. That’s not a simple fix.
References
- Kay SR, Fiszbein A, Opler LA. The Positive and Negative Syndrome Scale (PANSS) for Schizophrenia. Schizophrenia Bulletin, Volume 13, Issue 2, 1987, Pages 261-276
- Evensen J, et al. Flat affect and social functioning: A 10 year follow-up study of first episode psychosis patients. Schizophrenia Research, 2012
- Bowers D, Miller K, Mikos A, et al. Startling facts about emotion in Parkinson’s disease: blunted reactivity to aversive stimuli. Brain, Volume 129, Issue 12, December 2006, Pages 3356-3365
- Staring ABP, Van der Gaag M. Cognitive Behavioral Therapy for negative symptoms (CBT-n) in psychotic disorders: A pilot study. Journal of Behavior Therapy and Experimental Psychiatry, 2013
- Lincoln TM, et al. Negative Symptoms of Schizophrenia as Primary Target of Cognitive Behavioral Therapy: Results of the Randomized Clinical TONES Study. Schizophrenia Bulletin, 2012
- Granholm E, Holden J, Dwyer K, et al. Mobile-Assisted Cognitive Behavioral Therapy for Negative Symptoms: Open Single-Arm Trial With Schizophrenia Patients. JMIR Mental Health, 2020
- Maas AIR, Menon DK, Adelson PD, et al. Traumatic brain injury: integrated approaches to improve prevention, clinical care, and research. The Lancet Neurology, 2017