
Drug Interaction Checker – Avoid Risky Meds Mixes

Quick Takeaways
- A drug interaction is what happens when one substance another drug, a food, a supplement, alcohol, or even an underlying condition changes how a medication works in your body. Some interactions are harmless, a small percentage are dangerous, and the dangerous ones are what interaction checkers exist to catch.
- The highest-risk groups: older adults, anyone on five or more medications (polypharmacy), and patients with kidney or liver disease. DDI prevalence in chronic kidney disease patients runs between 56.9% and 89.1% in the published literature.
- Interactions fall into two mechanistic categories pharmacokinetic (the body’s handling of the drug changes) and pharmacodynamic (the drug’s effect at its target changes) and into five practical categories: drug-drug, drug-food, drug-supplement, drug-disease, and drug-alcohol.
- The combinations worth memorizing: warfarin + NSAIDs, SSRIs + tramadol/triptans/dextromethorphan, statins + macrolides or azoles, ACE inhibitors + potassium-sparing diuretics, opioids + benzodiazepines, grapefruit juice + many CYP3A4-cleared drugs.
- Free checkers (Drugs.com, Medscape, WebMD) are a useful first pass, but they disagree with each other on roughly 76–84% of SSRI-related interactions in published comparisons. Use two, then call the pharmacist.
- Around 6.5% of UK hospital admissions are tied to adverse drug reactions, and roughly one in six of those involve a drug-drug interaction (Pirmohamed et al., BMJ).
What are Drug Interactions?
A drug interaction occurs when another medicine, food, drink, supplement, herbal product, or coexisting illness alters the way a medication functions. Any alteration in a medicine’s effects brought on by recent or contemporaneous use of another medication, food, or dietary supplement is referred to as a drug interaction in the Merck Manual. In practical terms, the concept is considerably simpler: whatever you ingest, inject, inhale, or absorb has the potential to change the behavior of anything else you eat.
The change can be in any direction. Drug gets more powerful. The medicine gets weaker. The medicine is absorbed more quickly, more slowly or not at all. The medicine lingers in the bloodstream longer than it ought to. The medicine doesn’t function anymore. Or two drugs that are safe on their own combine to create a new side effect that neither would create on its own haemorrhage, sedation, a severe spike or drop in blood pressure, a confused mental state.
Most interactions sit somewhere on the harmless-to-mildly-annoying end of the spectrum. The clinically meaningful share is smaller, but it’s the share that matters. Pirmohamed’s BMJ analysis of 18,820 UK hospital admissions found 6.5% were related to adverse drug reactions, with interactions accounting for around one in six of those aspirin with warfarin causing GI bleeding, NSAIDs combined with diuretics or ACE inhibitors causing renal failure, that kind of thing. A 2024 cross-sectional study in Scientific Reports put the rate of emergency hospital admissions caused by adverse drug reactions at 5.0% in a population with a median age of 78. The Dechanont systematic review surfaced an even more striking number for the at-risk subgroup: among patients already experiencing an adverse drug reaction, drug-drug interactions were behind 22.2% of admissions.
That’s the population-level picture. At the individual level, you don’t get to know in advance whether you’re in the 1% that runs into a serious interaction or the 99% that doesn’t. Which is the reason the checking is worth the two minutes.
Who’s at Risk for Drug Interactions?
Everyone who takes more than one medication, in principle. But the risk isn’t evenly distributed, and several factors push it up sharply.
- Elderly people’s body composition, liver enzyme activity, renal filtration, and the distribution of medications in tissue are all affected by aging. Over 70% of those over 70 take at least one prescription, and the percentage for five or more rises significantly with each additional decade. Adults exposed to six or more of the most frequently implicated medications had roughly 7.5 times higher odds of being hospitalized due to an adverse drug reaction than those exposed to none, according to an English study published in Pharmacoepidemiology and Drug Safety in 2024 that examined primary care and hospital data for individuals aged 65 to 100.
- Anyone on five or more medications (polypharmacy). This is the single most important risk factor and it shows up across nearly every study on the topic. A cross-sectional analysis of drug therapy prescribed at hospital discharge for older adults found polypharmacy was independently associated with potential drug interactions at an odds ratio of 12.62 far larger than the effect of age, sex, or any individual comorbidity.
- Patients with chronic renal illness. The kidneys excrete most medications to a significant extent. Impaired clearance affects concentrations throughout the entire prescription list all at once. CKD patients are generally on many medications to start with, because of the conditions that travel with kidney disease hypertension, diabetes, cardiovascular disease. Published DDI prevalence in individuals with CKD ranged from 56.9% to 89.1%, closer to “essentially everyone” than “a high-risk subgroup.”
- those suffering from liver illness. The cytochrome P450 enzyme system in the liver is responsible for the majority of metabolic drug clearance. Drug metabolism is altered, sometimes significantly, by cirrhosis, hepatitis, fatty liver, and any other illness that affects liver function.
- individuals with endocrine disorders such as hypothyroidism and diabetes. In addition to polypharmacy, the aforementioned discharge research identified hypothyroidism (OR 7.29) and diabetes (OR 2.16) as independent risk factors for possible medication interactions. Levothyroxine itself interacts with a wide range of popular medications and supplements, which contributes to the larger prevalence of hypothyroidism.
- High risk drug classes. If one of the drugs you are taking is heavily involved in drug interactions, you are naturally at higher risk. Warfarin is the textbook narrow therapeutic index , hundreds of documented interactions . Other drugs in this group include antiepileptics such as phenytoin and carbamazepine, some antibiotics such as rifampicin and clarithromycin, immunosuppressants such as cyclosporine and tacrolimus, and a handful of the SSRIs (fluoxetine and fluvoxamine in particular).
- Pregnant women, children, and people with rare pharmacogenetic variants. Smaller groups, but real ones, and they’re systematically underrepresented in the trial data that interaction databases are built from meaning a checker may give them the same answer it gives an average 40-year-old when the right answer is different.
If you’re in more than one of these categories at once, the risk doesn’t add. It multiplies. An 80-year-old on eight medications with stage 3 CKD isn’t twice as likely to run into a clinically meaningful interaction as someone with one risk factor they’re in a different category entirely.
What Are the Different Types of Drug Interactions?
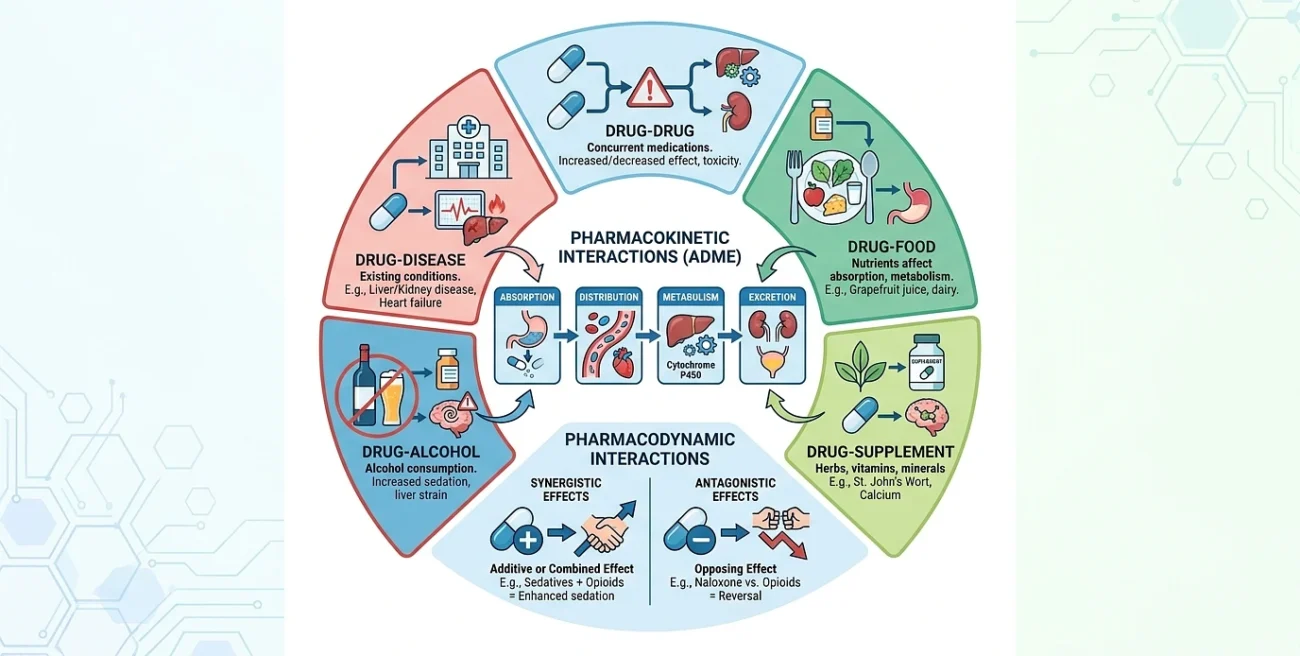
There are two useful ways to slice the category. The first is by what’s interacting (drug, food, supplement, condition, alcohol). The second is by how the interaction works at the biological level (pharmacokinetic vs. pharmacodynamic). Both are worth understanding.
By what’s involved
Drug-drug interactions. Two or more medications taken together, with one changing the effect of another. This is the category most checkers focus on and the one most patients think of first. Warfarin plus aspirin. SSRI plus tramadol. Simvastatin plus clarithromycin. The major pharmacy databases Lexicomp, Micromedex, Drugs.com are built primarily around this category.
interactions between drugs and food. Food alters the metabolism, action, or absorption of drugs. The most well-known example is grapefruit juice, which significantly inhibits the CYP3A4 enzyme, causing blood levels of several statins, calcium channel blockers, and immunosuppressants to increase many times. Less well-known: high-fat meals can significantly alter the absorption profile of some HIV antiretrovirals; tyramine-rich foods (aged cheese, cured meats, fermented soy) can cause hypertensive crises in patients on MAOIs; leafy greens high in vitamin K counteract the anticoagulant effect of warfarin; and dairy products bind to tetracycline and fluoroquinolone antibiotics and block their absorption.
interactions between drugs and supplements. Because supplements may be obtained without a prescription and because the term “natural” doesn’t seem dangerous, this is the group that patients underestimate the most. Strong CYP3A4 inducers like St. John’s Wort may reduce the effectiveness of immunosuppressants, warfarin, certain HIV antiretrovirals, and oral contraceptives. When used with anticoagulants, ginkgo biloba has an additional antiplatelet effect. Large amounts of garlic and fish oil increase the risk of bleeding. Supplements including calcium and iron have been shown to bind with levothyroxine and certain antibiotics in the intestines. Because it came from a health food shop, the danger does not go away.
interactions between drugs and diseases or conditions. When an underlying illness is present, a medicine that is harmless in a healthy individual becomes hazardous. NSAIDs lead to issues with CKD and heart failure. Beta-blockers may exacerbate asthma and conceal hypoglycemia in diabetics. In hypertensives, decongestants may cause blood pressure spikes. Anticholinergics exacerbate benign prostatic hyperplasia and narrow-angle glaucoma. Since there isn’t a second drug involved, the drug interacting with you doesn’t appear on most drug-drug checks.
Alcohol-drug interaction. Alcohol competes with many drugs in the same metabolic pathways, irritates the lining of your stomach, stresses your liver, and is a sedative. Alcohol and paracetamol are the most hazardous combos (hepatotoxicity). even at the specified limit if frequent drinking occurs. Alcohol with painkillers or benzodiazepines (respiratory depression). Alcohol with disulfiram or metronidazole (strong nausea, vomiting, and disulfiram response flushing). Alcohol with sulfonylureas or insulin (hypoglycemia). Most antidepressants plus alcohol (additive sedation and impaired judgment).
By how the interaction works
Pharmacokinetic interactions One medicine alters how the body absorbs, distributes, metabolises or excretes another, the four phases summarised by the acronym ADME. These effects generally foreseeable given the known enzyme profile of a medicine and commonly involve the CYP450 system in the liver. Clarithromycin inhibits CYP3A4 and increases the blood levels of simvastatin (risk of rhabdomyolysis) Rifampicin induces multiple CYP enzymes and decreases the blood levels of oral contraceptives to the extent that pregnancy may result Antacids and proton pump inhibitors increase the pH in the stomach and decrease the absorption of drugs that require an acid environment for absorption (ketoconazole, some HIV drugs, iron salts)
Pharmacodynamic interactions. Two medications are acting on the same biological target, either piling on (additive or synergistic impact) or cancelling each other out (antagonism). The benzodiazepine-opioid problem: two CNS depressants taken together produce greater drowsiness than either alone. Two potassium-lowering medicines taken together lower potassium more than each alone. Two medications that increase serotonin ( SSRI + tramadol , SSRI + MAOI , SSRI + St. John’s Wort ) drive serotonin levels into the danger zone serotonin syndrome .
Pharmaceutical (incompatibility) interactions. Less commonly discussed at the patient level because these mostly happen before the drug enters the body two IV medications mixed in the same line that precipitate out, for example, or a drug that becomes inactive when added to a particular diluent. Relevant in hospitals; rarely relevant at home.
What are Common Drug Interactions?
The combinations below come up most consistently in clinical literature and in the regulatory safety bulletins from the FDA, the MHRA, and the pharmacy professional bodies. These are the ones worth recognizing on sight.
Anticoagulants and antiplatelets
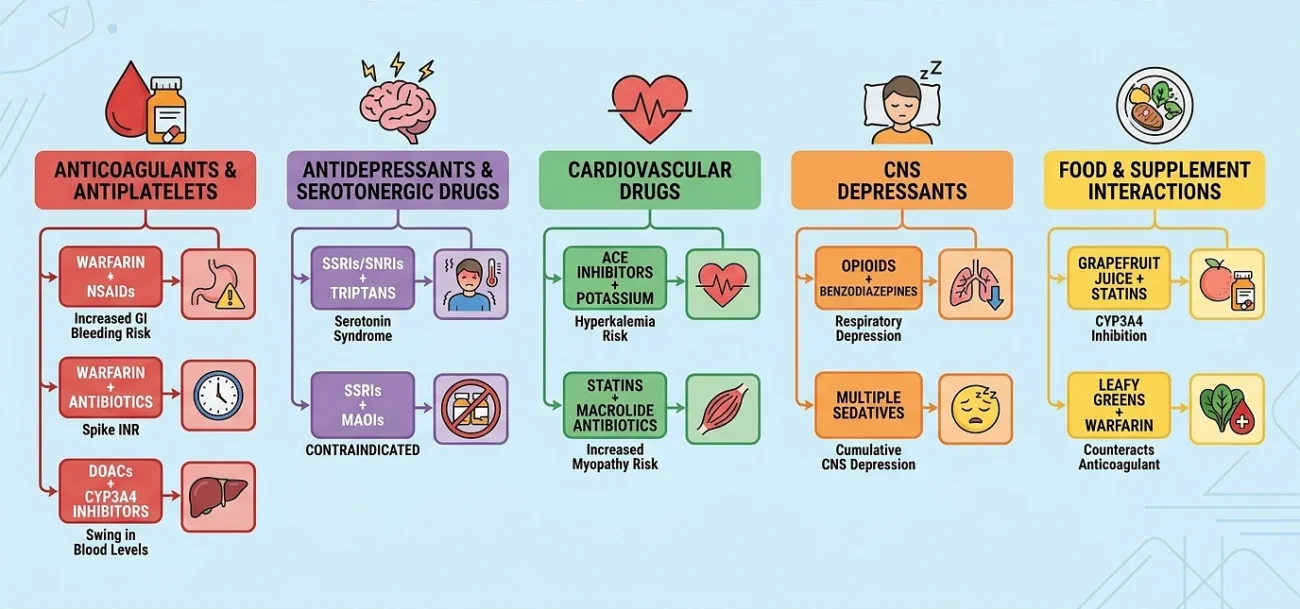
- NSAIDs (ibuprofen, naproxen, diclofenac, ketorolac) and warfarin significantly increase the risk of gastrointestinal bleeding. Warfarin inhibits clotting, whereas NSAIDs harm the intestinal lining. The combination has been linked to deadly bleeding incidents.
- Warfarin with SSRIs, especially fluoxetine and fluvoxamine: SSRIs cause platelet aggregation, and fluoxetine and fluvoxamine both block the metabolism of warfarin via CYP2C9 and 1A2, which is a double bleeding hit. The safest SSRIs for those on warfarin are citalopram and sertraline.
- Warfarin + antibiotics, especially metronidazole, trimethoprim-sulfamethoxazole, fluconazole, and ciprofloxacin: can spike INR within days. Many warfarin patients on antibiotics need an INR check 3–5 days into the course.
- Warfarin + acetaminophen at regular daily doses: the underappreciated one. Acetaminophen is the recommended analgesic for warfarin patients over NSAIDs, but regular daily use does raise INR. An INR check 3–5 days after starting daily acetaminophen is the usual precaution.
- DOACs (apixaban, rivaroxaban, dabigatran) + strong CYP3A4 or P-glycoprotein inhibitors/inducers (clarithromycin, ketoconazole, rifampicin, phenytoin, carbamazepine): blood levels can swing in either direction, leading to bleeding or to thrombosis.
- Aspirin + clopidogrel continued past the indicated duration: dual antiplatelet therapy raises bleeding risk significantly.
Antidepressants and Serotonergic Drugs
- Triptans, tramadol, dextromethorphan, linezolid, and St. John’s Wort combined with SSRIs and SNRIs result in serotonin syndrome. Within hours of the second dosage, symptoms include agitation, fever, sweating, tremor, hyperreflexia, and tachycardia. Most cold syrups you can buy at the counter have the cough suppressant dextromethorphan, which is the portion most patients miss.
- SSRIs + MAOIs (phenelzine, tranylcypromine, selegiline): contraindicated. Fluoxetine has a long half-life, so the washout period before starting an MAOI is roughly five weeks.
- SSRIs + NSAIDs: independently increases upper GI bleeding risk, flagged by Mayo Clinic and supported by multiple meta-analyses.
Cardiovascular Drugs
- ACE inhibitors / ARBs + potassium-sparing diuretics (spironolactone, eplerenone) or potassium supplements: hyperkalemia, sometimes severe enough to cause cardiac arrhythmias or arrest. The risk is higher in CKD patients and in older adults.
- Beta-blockers + non-dihydropyridine calcium channel blockers (verapamil, diltiazem): profound bradycardia or AV block.
- Statins + macrolide antibiotics (clarithromycin, erythromycin) or azole antifungals (itraconazole, ketoconazole): raises statin blood levels via CYP3A4 inhibition, increasing the risk of myopathy and rhabdomyolysis. Simvastatin and lovastatin are the most affected; pravastatin and rosuvastatin much less so.
- Digoxin + amiodarone, verapamil, or clarithromycin: digoxin levels can climb into the toxic range.
CNS Depressants
- Opioids + benzodiazepines: respiratory depression. This combination appears in a substantial share of accidental overdose deaths in the US, which is why the FDA carries a black-box warning on it.
- Opioids + gabapentin or pregabalin: also causes respiratory depression; risk has been rising as gabapentinoid prescribing has climbed over the last decade.
- Multiple sedatives stacked (benzodiazepine + Z-drug + alcohol + sedating antihistamine): cumulative CNS depression that’s more than additive.
Antibiotics and Contraception
- Rifampicin and rifabutin + oral contraceptives: enzyme induction drops contraceptive blood levels enough to cause breakthrough ovulation. Backup contraception is required during use and for several weeks after.
- Most other antibiotics + oral contraceptives: contrary to long-standing patient lore, most antibiotics do not meaningfully reduce contraceptive efficacy. Rifampicin and a handful of related enzyme inducers are the exception, not the rule.
Diabetes Medications
- Sulfonylureas (glipizide, glyburide) + alcohol, beta-blockers, or certain antibiotics: hypoglycemia.
- Metformin + iodinated contrast media (used in CT scans): risk of contrast-induced nephropathy and, rarely, lactic acidosis. Most protocols hold metformin around the procedure.
Food and Supplement Interactions
- Grapefruit juice + statins, certain calcium channel blockers (felodipine, nifedipine), tacrolimus, cyclosporine, some benzodiazepines: CYP3A4 inhibition, raising drug levels. The effect of grapefruit is dose-dependent and can last 24+ hours, which means spacing doses out doesn’t reliably fix it.
- Leafy greens (kale, spinach, broccoli) + warfarin: vitamin K counteracts the anticoagulant effect. Consistency matters more than avoidance sudden changes in green vegetable intake destabilize INR more reliably than a steady high intake.
- Dairy and calcium-fortified products + tetracyclines, fluoroquinolones, levothyroxine, bisphosphonates: binding in the gut reduces absorption. Typical advice is to space doses by at least 2–4 hours.
- St. John’s Wort + oral contraceptives, warfarin, immunosuppressants, certain antiretrovirals, certain chemotherapy agents: enzyme induction reduces drug levels and clinical efficacy.
- Ginkgo, garlic, ginger, high-dose fish oil + anticoagulants or antiplatelets: additive bleeding risk.
Where the Checkers Help, and Where They Don’t
A drug interaction checker is the cheapest first-pass safety net you have. The major free tools Drugs.com, Medscape, WebMD let you enter your full medication list, including OTC products and supplements, and return a categorized list of potential interactions in under a minute.
The catch: the tools don’t agree with each other. A 2025 analysis of how five popular checkers handled SSRI interactions found agreement on only 16–24% of the interactions identified (Gwet’s AC1 = 0.16–0.24). In oncology comparisons, Lexicomp and Drugs.com scored highest in sensitivity; RxList came out near the bottom. Medscape covers around 9,200 drugs but is written for clinicians the language assumes you know what CYP3A4 induction or pharmacodynamic antagonism mean.
A reasonable home workflow:
- Run your list through Drugs.com first. Its food, alcohol, and condition coverage is broader than most.
- For anything flagged as major or severe, cross-check with Medscape or WebMD.
- If two tools disagree on something serious, call the pharmacist. They have access to the subscription-grade databases (Lexicomp, Micromedex usually thousands of dollars per year for institutional access) that hospitals use, and they can factor in your dose, your kidney function, and your other conditions in a way no automated tool can.
The no-checker doesn’t take into consideration your particular dose, your renal function, your hepatic function, your age, your weight, your pharmacogenetic variations, the time between doses, or what you’ve actually been taking vs. what is in your record. A checker that indicates a “major” interaction may be flagging something that’s clinically worthless at your dose; a checker that gives you the all-clear may be missing something that only matters in your individual case.
What to do in Practice
- Keep one written list of everything you take prescriptions, OTC products, vitamins, herbal supplements, CBD, recreational substances you’re honest about. Update it when something changes, bring it to every appointment.
- Use one pharmacy if you can. A single pharmacy record triggers automatic interaction checks every time you fill something new. Splitting between two or three pharmacies for cost reasons, which a lot of people do, defeats that built-in safety net.
- Ask about food interactions when starting any new medication. Grapefruit, dairy, leafy greens, alcohol these don’t always make it into the standard counseling at the pickup window.
- Watch the first two weeks of any new medication for unusual symptoms bleeding, bruising, confusion, racing heart, muscle pain, fever without infection, unusual fatigue. New interactions usually show up early.
- Call the pharmacist before the ER for mild symptoms or general questions. Call the ER (or 911) for difficulty breathing, severe bleeding that won’t stop, chest pain, very high fever with muscle rigidity, loss of consciousness, or signs of an allergic reaction like throat swelling.
A drug interaction checker is the cheapest insurance policy in medicine free, instant, and most of the time it tells you ou’re fine. The small percentage of the time it doesn’t, it’s the difference between a normal week and a hospital admission. Use it. Then call the pharmacist anyway.
Sources
- Pirmohamed M et al. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18,820 patients. BMJ.
- Staa TP et al. (2024). Adverse drug reactions and hospital admissions: large case-control study of patients aged 65–100 years using linked English primary care and hospital data. Pharmacoepidemiology and Drug Safety.
- Dechanont S et al. (2014). Hospital admissions/visits associated with drug-drug interactions: a systematic review and meta-analysis. Pharmacoepidemiology and Drug Safety.
- Hughes JE et al. (2024). Drug-drug interactions and the risk of adverse drug reaction-related hospital admissions in the older population. British Journal of Clinical Pharmacology.
- Prevalence of urgent hospitalizations caused by adverse drug reactions: a cross-sectional study. Scientific Reports (Nature), 2024.
- Drug-drug interactions in polypharmacy patients: the impact of renal impairment. PubMed Central.
- Potential drug interactions in drug therapy prescribed for older adults at hospital discharge: cross-sectional study. PubMed Central.
- Mayo Clinic: Selective serotonin reuptake inhibitors (SSRIs).
- Merck Manual Professional Edition: Drug Interactions.
- ScienceDirect Topics: Drug Interaction — overview.
- Pharmacy Times: 10 Drug Interactions Every Pharmacist Should Know.