
Gum Cancer: Causes, Symptoms and Treatment
Gum cancer is one of the forms of oral cancer, which usually starts in the surface cells. Mainly caused by tobacco use, heavy alcohol consumption and HPV infections. If the disease is caught early during routine dental check-ups or patients notice persistent mouth sores, it is very treatable.
The Reason It’s So Easy to Miss
Most oral cancers form on the tongue. This one is the unusual exception, and that rarity is part of the problem. Gingival squamous cell carcinoma accounts for around 6% of all oral malignancies, and because it mimics the characteristics of a wide variety of common diseases and abnormalities, it’s a genuinely challenging cancer for a physician or pathologist to diagnose.
The trap is that it doesn’t announce itself. The early signs – sores, white patches, bleeding, and pain or numbness on the can mimic those of gingivitis or tooth infection. A person notices a sore patch, assumes it’s an ordinary gum cancer issue, waits for it to clear, and by the time it doesn’t, the disease has had weeks or months to grow.
There’s a second complication specific to this malignancy. While many medical studies confirm a strong link between smoking and oral cancer in general, gingival squamous cell carcinoma has only a minor association with smoking, which makes it even harder to detect because it often appears in people who don’t fit the usual risk profile. Someone who has never smoked may not think “cancer”, and neither might their clinician.
What This Cancer Actually Is
Gingival cancer is a malignant tumor that develops in the tissue of the upper or lower jaw. About 95% of the time, it’s a squamous cell carcinoma, which arises from the flat squamous cells lining the mouth.
- Mandibular type – found in the lower gum cancer. This is more common than the upper-jaw form, and tobacco irritating the soft tissue covering the lower mandible, causing chronic trauma, is one route to it.
- Maxillary type – found in the upper jaw, the maxilla. Less common than the mandibular form.
A point worth holding onto, because it changes how seriously early signs should be taken: the size of the tumor does not always predict how aggressively it will spread, and the disease can extend into nearby structures such as the sinuses or jawbone.
What Raises the Risk
The recognized contributors include:
- Tobacco in all forms – smoking, chewing tobacco, and snus. This is the strongest general oral-cancer risk factor, though as noted, its link to gingival disease specifically is weaker than for other oral cancers.
- Alcohol use – a well-established independent risk factor for oral cavity cancers, and the risk compounds when combined with tobacco.
- Poor oral hygiene – listed alongside tobacco and alcohol as a primary risk factor for the precancerous lesions that can develop into malignancy.
- Age and sex – gingival squamous cell carcinoma is more common in white men after the age of 40.
- Precancerous lesions – white or red patches that can turn malignant over time, covered in detail below.
The Precancerous Patches That Come Before

Some of these tumors begin as visible patches that aren’t yet cancer but carry a real chance of becoming it. Catching these is one of the clearest opportunities for early intervention.
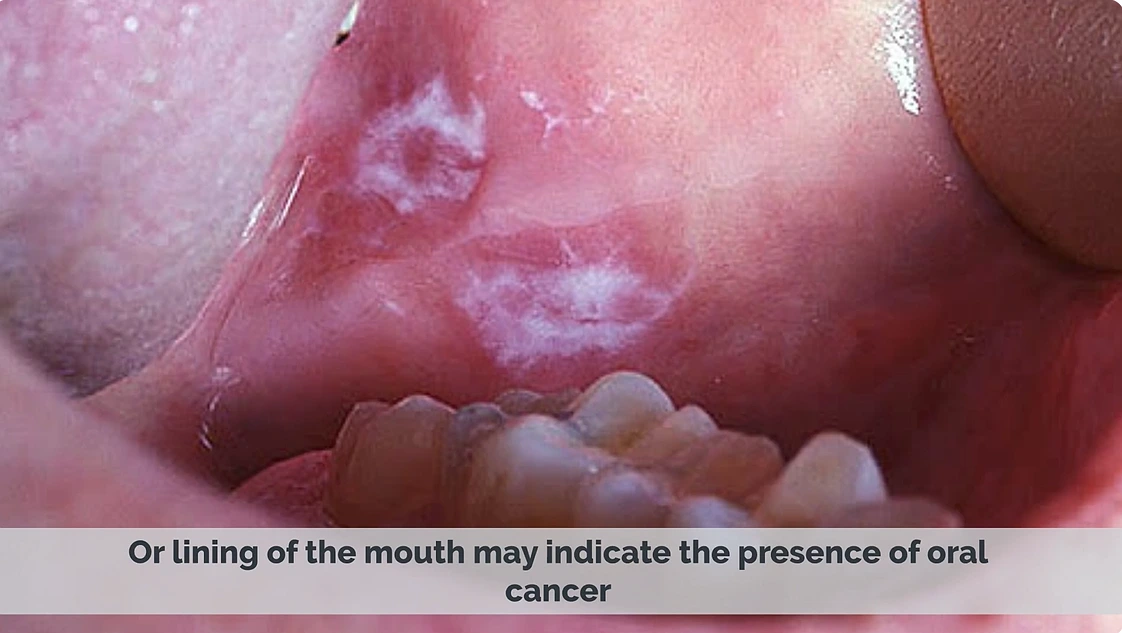
Leukoplakia (white patches):
Leukoplakia appears as white patches that cannot be wiped off and may cover certain areas or the entire lining of the mouth. Depending on the specific form, three to 38 percent of leukoplakia cases develop into squamous cell carcinoma if left untreated. It’s linked to tobacco, alcohol, and poor oral hygiene.
Erythroplakia (red patches):
This one is rarer but far more dangerous. Erythroplakia presents as velvety, bright dark-red patches on the lining of the mouth. It’s much rarer than leukoplakia, but if left untreated, 90 percent of erythroplakia cases develop into cancer.
That 90% figure is the reason any persistent red patch on the deserves prompt professional attention rather than a wait-and-see approach. Red patches are often one of the first warning signs.
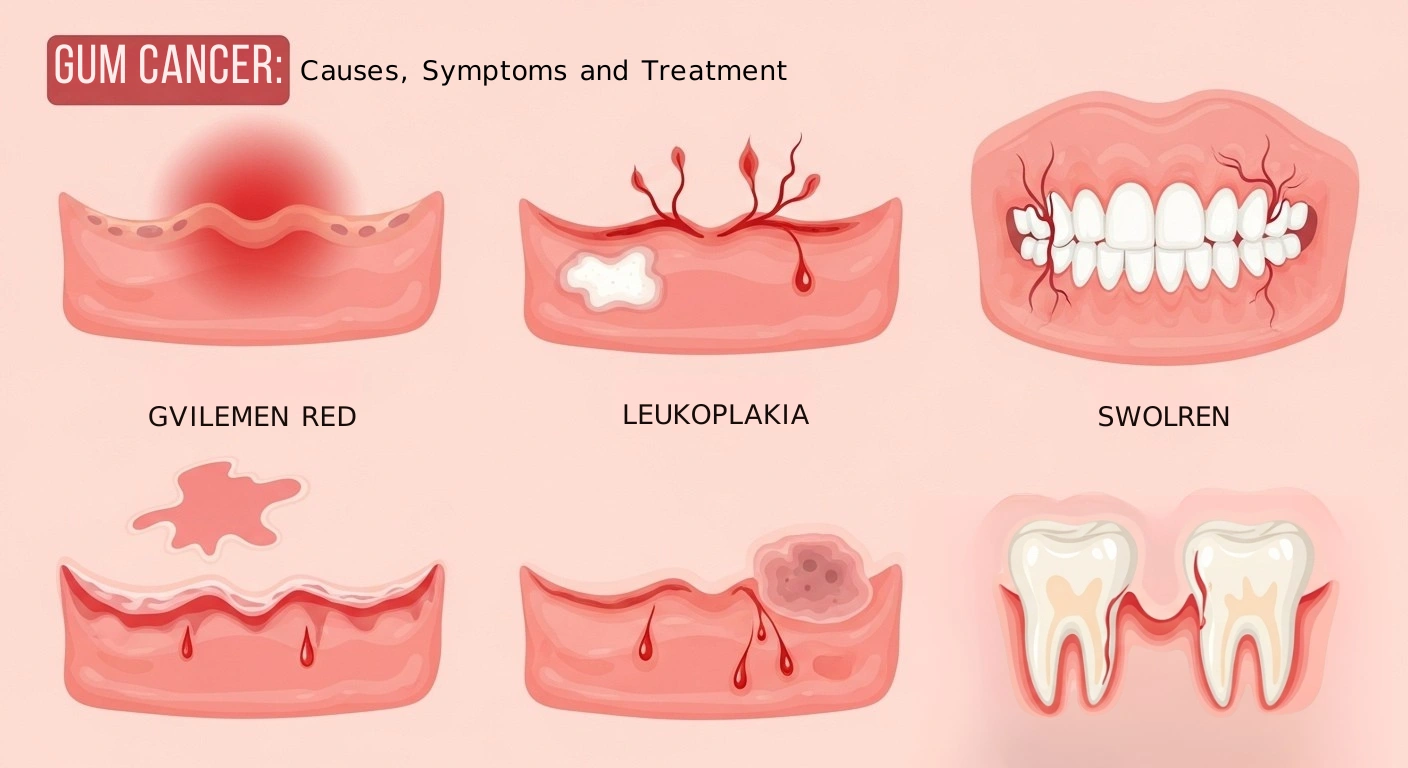
Symptoms That Should Not Be Ignored
The difficulty, again, is that these overlap with harmless conditions. The deciding factor is usually persistence – ordinary gum problems resolve, malignancy doesn’t. Watch for:
- Sores that don’t heal – sores on the recognized sign, and spindle cell cancer in particular can look like an ulcer that doesn’t heal.
- White or red patches – the leukoplakia and erythroplakia described above.
- Bleeding from the that isn’t explained by brushing or known disease.
- Pain or numbness in the gums. Numbness on the a specific sign worth noting, since ordinary irritation doesn’t usually cause it.
- A lump, swelling, or growth. The tumor either grows outward as an ulcer that initially looks like a swelling, or it grows inward, creating a crater-like depression.
- A velvety or warty bump – the appearance verrucous tumors can take.
How It’s Diagnosed
The first line of detection is often a routine dental visit, which is one of the strongest arguments for not skipping checkups. A dentist can often spot it using a small mirror and a light to examine, checking the color inside the mouth for any white or red patches, lumps, or sores.
When something suspicious is found, diagnosis is confirmed with a biopsy – a small tissue sample examined for malignant cells. Imaging such as CT or MRI scans then determines how far it has spread, which sets the stage and guides treatment.
Staging follows tumor size and spread:
- Stage 1 – the tumor is up to 2 cm with no lymph node involvement.
- Stage 2 – the tumor is between 2 and 4 cm and has not spread into the regional lymph nodes.
- Stage 3 – the tumor is larger than 4 cm, or it has spread to surrounding lymph nodes.
- Stage 4 – often called metastatic, it invades large lymph nodes, distant organs, and grows deep into the tissue.
Treatment Options by Stage
Surgery:
The cornerstone of treatment, especially for early-stage disease. Surgery is the primary treatment for early squamous cell carcinoma of the gum, allowing for preservation of speech, swallowing, and appearance. In more advanced cases the surgery is more extensive. It’s usually treated with surgery, which may include removal of parts of the jawbone and some teeth.
Radiation therapy:
Used either as a follow-up to surgery or as a primary approach in certain cases. In oral cancer management, external beam radiation is the most common technique, and it’s particularly important when the surgical margins of removal were not sufficient – meaning it targets any cancer cells that may remain at the edges of where the tumor was removed.
Chemotherapy
After the tumor is removed via surgery, a doctor may recommend chemotherapy or radiation therapy as a follow-up to help kill any cancer cells left behind. It’s frequently combined with radiation in advanced cases.
Combined chemoradiotherapy:
For locally advanced disease, the two are often delivered together. Concurrent chemoradiotherapy is an important treatment for locally advanced head and neck squamous cell carcinoma, because it can preserve organ and function integrity while improving the local control rate.
Newer and targeted approaches:
For patients who can’t undergo surgery, or whose cancer has specific genetic features, additional options are emerging. Immunotherapy has been used to maintain quality of life with minimal side effects in older patients who chose to avoid surgery due to age and other health conditions. Targeted therapy is still developing. It remains in the exploratory stage for gingival carcinoma, though there are documented cases of advanced disease responding to targeted drugs combined with chemoradiotherapy.
Survival and Why Early Detection Changes Everything
The overall numbers are moderate, but they shift dramatically with stage. The 5-year survival rate is around 68%, and it differs significantly by stage, with localized tumors having a much higher survival rate.
That gap between localized and advanced disease is the entire reason this article exists. The broader oral-cancer picture underlines the cost of late detection. Across squamous cell carcinoma of the head and neck, only about one-third of patients are diagnosed during the early stage, and nearly half of patients ultimately die due to tumor-related complications.
This article is for informational purposes only and does not constitute dental or medical advice. If you notice any gum sore, patch, lump, or numbness that persists beyond two weeks, see a dentist or doctor for evaluation.
References:
- Alqahtani et al. “Managing misdiagnosed gingival squamous cell carcinoma (GSCC) with occult symptoms: A report of two cases.” Annals of Medicine and Surgery, ScienceDirect. 2021.
- “Squamous Cell Carcinoma of Left Buccal Alveolar Ridge.” NCBI PMC.
- “Case report: Prompt response to radiotherapy and chemotherapy combined with crizotinib in gingival sarcomatoid squamous cell carcinoma with MET 14 mutation.” NCBI PMC.