
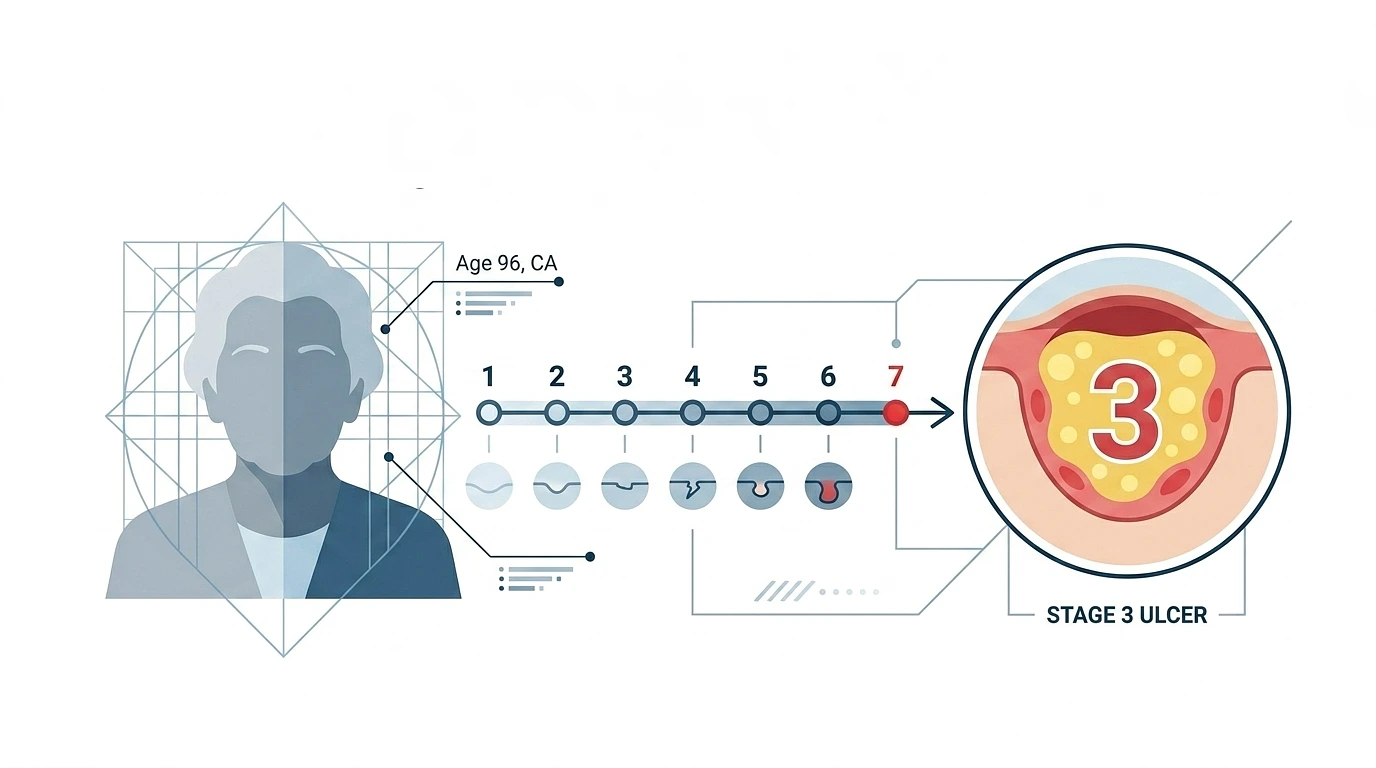
A 96-Year-Old California Woman Developed a Stage 3 Pressure Ulcer in a Week. The Medical Pattern Behind What Happened.
Ruby Evans was 96 and recovering from a stroke. Her family checked her into Windsor Vallejo Care Center in Vallejo for a short-term rehabilitation stay. Standard arrangement, the kind families set up after a stroke when home recovery is not yet practical. Because she was immobile, her care plan specifically required repositioning every two hours to prevent skin breakdown. Within a week she had developed a stage 3 pressure ulcer. She died shortly after, and in January 2026 a Solano County jury awarded her family $15.75 million, finding the facility liable for elder abuse and wrongful death.
What made the verdict unusual was not the bedsore. It was what the jury concluded about the documentation. The facility’s records showed care that had been performed. The wound on Ruby’s body showed care that had not. The jury found that the records were falsified.
What A Stage 3 Pressure Ulcer Actually Is
For anyone who has not been close to long-term care, the staging system is worth understanding because it tells you exactly how long the neglect went on.
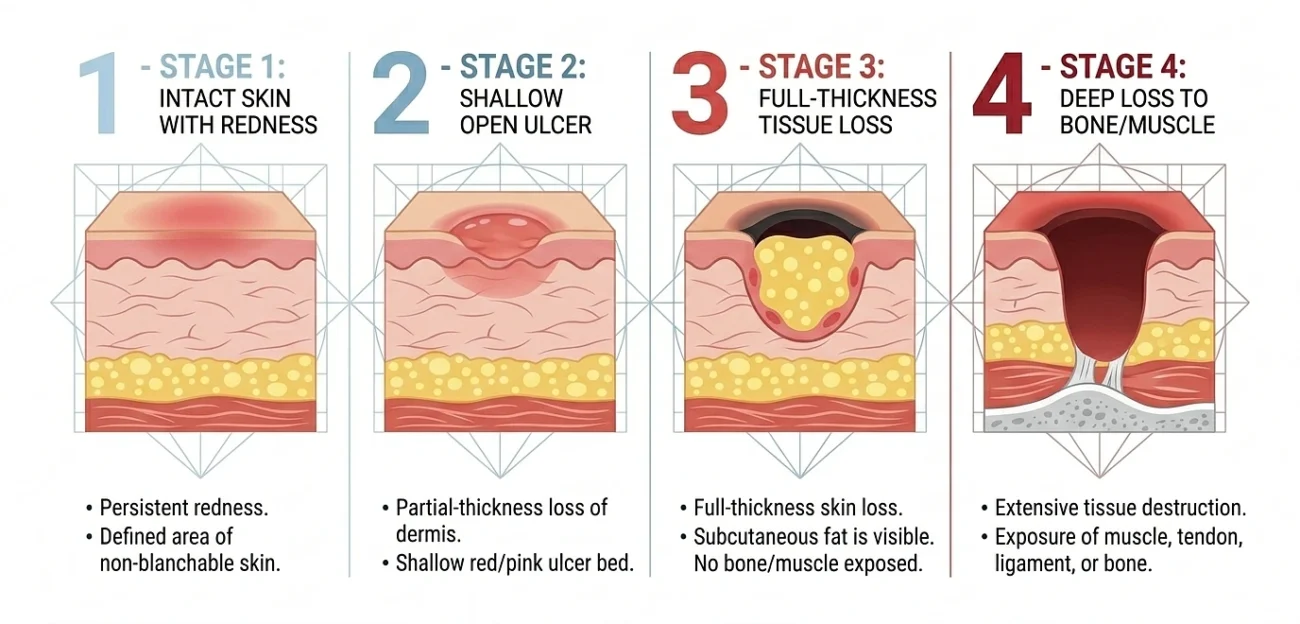
Pressure ulcers, also called pressure injuries or bedsores, form when skin and underlying tissue lose blood supply from sustained pressure. The clinical staging system runs from Stage 1 through Stage 4:
- Stage 1. Skin is intact but persistently red, the area does not blanch when pressed. Reversible if pressure is relieved.
- Stage 2. Partial thickness skin loss. A shallow open wound or blister. Still relatively early.
- Stage 3. Full thickness skin loss. The wound extends down through the dermis and into the subcutaneous fat. Visible fat tissue. This is the stage Ruby reached in one week.
- Stage 4. Full thickness loss with exposed muscle, tendon, or bone. Often with infection extending into deeper structures, including osteomyelitis.
A stage 3 wound is not a minor injury. It is a deep tissue loss that requires weeks to months of medical management, often with surgical debridement, sometimes with flap reconstruction. In a 96-year-old stroke patient it is also frequently fatal, because the wound becomes a portal for bloodstream infection, and the elderly immune system handles sepsis poorly.
The other thing the staging tells you is the timeline. A stage 3 wound does not develop overnight. Skin breakdown progresses through the earlier stages first, which means the redness, the partial-thickness break, the deeper involvement, all of it was visible to anyone who looked.
What The Care Plan Was Supposed To Prevent
The two-hour repositioning protocol is not arbitrary. It comes from decades of clinical research on tissue ischemia. When an immobile patient lies in one position, the soft tissue compressed between bone and bed surface loses blood supply, and after roughly two hours the tissue starts to suffer ischemic damage. Reposition before that window closes and the tissue recovers. Leave the patient in one position for four, six, eight hours and the damage accumulates faster than the body can repair it.
For a stroke patient who cannot reposition herself, the entire prevention strategy rests on staff actually performing those scheduled turns. The two-hour clock starts running the moment the resident is positioned, and someone has to be the one to come into the room and move her.
The protocol is simple to write into a care plan. It is harder to execute consistently when the unit is understaffed. A typical certified nursing assistant on a busy long-term care floor might be responsible for eight to twelve residents at once, each of whom needs repositioning, toileting, feeding assistance, and basic hygiene. If the staffing ratio is wrong, scheduled turns get missed. Once they start getting missed, the pressure injury cascade begins.
The Medical Signs The Family Probably Never Saw
This is the part worth dwelling on because it explains why so many cases like Ruby’s go undetected until the wound is already serious.
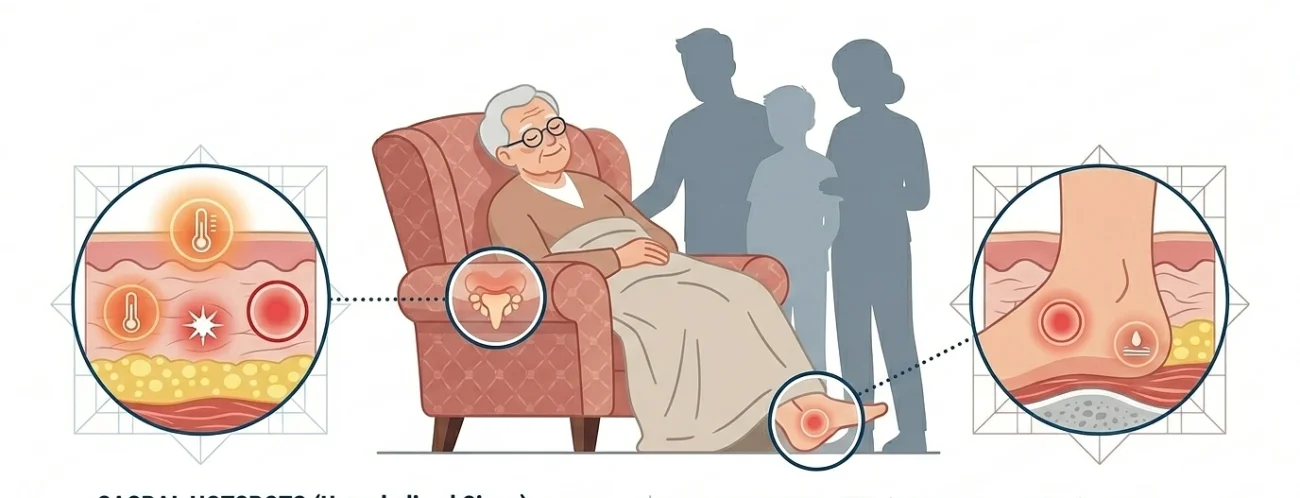
Families visiting nursing home residents usually see the resident dressed, in bed or in a chair, blanket pulled up to the shoulders or waist. The sacrum, the heels, the back of the head, the hips, the ischial tuberosities at the base of the buttocks, all the high-risk pressure points sit underneath clothing or bedding. A stage 1 redness or a stage 2 blister is not visible during a typical visit.
What is sometimes visible:
- A persistent low-grade fever without an obvious source, which can be the body responding to early tissue damage or infection at the wound site.
- Loss of appetite that develops over a few days, which often accompanies the metabolic stress of a healing or infected wound.
- Withdrawal or unusual quietness in a resident who was previously more engaged, sometimes a response to pain that the resident cannot fully articulate.
- A new smell when the family is close to the resident, which can be the wound, particularly once infection sets in.
- Reluctance to move or be moved, which can be the resident protecting a painful area.
None of these are diagnostic on their own. Together, and in a resident at high risk for skin breakdown, they should prompt the family to ask whether the resident has been examined for pressure injuries, and to request to see the skin assessment from the most recent nursing review.
What The Records Said Versus What The Wound Showed
The most damning element of the Ruby Evans case, the part that pushed the verdict to $15.75 million with significant punitive damages, was the documentation discrepancy.
Skilled nursing facilities are required to maintain detailed records of repositioning, skin assessment, wound staging, and care interventions. Those records are supposed to be the contemporaneous account of what actually happened in the room. In Ruby’s case, the records showed repositioning being performed on schedule and skin assessments being conducted regularly. The wound on her body was incompatible with that documentation. A stage 3 pressure ulcer in one week is not what the recorded care would have produced.
The jury concluded that the records had been falsified to cover the gap between what was supposed to happen and what actually did. Once the documentation itself becomes the evidence of cover-up, the case moves from negligence into the higher-tier elder abuse category that California’s Welfare and Institutions Code section 15657 specifically targets, which is part of why the verdict included punitive damages.
For families of other residents, the lesson is that the medical record is not always a reliable account of what happened, especially in facilities with chronic staffing problems and a culture of paper compliance.
The Wider California Pattern
Ruby’s case is not isolated. The State of California filed a separate lawsuit in June 2025 against Sweetwater Care, a Carlsbad-based nursing home chain, after state investigators documented more than 25,000 violations across the chain’s facilities between 2020 and 2024. The investigators found that the company had operated below legal staffing levels for years while collecting more than $196 million in Medi-Cal funding. The harms documented in the investigation included untreated bedsores, delayed medical care, and unattended falls.
In March 2026, a separate California case produced a $110 million verdict against the operators of Greenhaven Estates Assisted Living and Memory Care after a resident with dementia walked out an exit door and died of hypothermia in 38-degree weather. The trial revealed a pattern of cost-cutting that left residents at serious risk in pursuit of higher returns.
The thread connecting these cases is not bad individual workers. It is systemic understaffing driven by ownership structures that treat skilled nursing as a revenue engine rather than a clinical service. When the staffing ratio is wrong, scheduled care does not happen. When scheduled care does not happen, the predictable medical injuries follow.
What Families Can Actually Do During A Stay
A few specific actions during a loved one’s stay matter more than people realize.
Ask for the skin assessment
California facilities are required to perform regular skin assessments on residents at high risk for pressure injuries. Families have the right to request to see these assessments. If the documentation is vague, incomplete, or the staff is reluctant to produce it, that is a signal.
Check the high-risk areas yourself
With the resident’s permission and dignity in mind, look at the sacrum, heels, hips, and the back of the head during visits. Pressure injuries are not always painful in their early stages, particularly in residents with reduced sensation, so the resident may not report them even when they exist.
Watch the staffing patterns
How long does it take for a call light to be answered. How many residents is each certified nursing assistant covering. How often does anyone come into the room during a long visit. These are the operational signals of whether the staffing supports the care the facility promised.
Verify the facility’s CDPH history
The California Department of Public Health publishes inspection reports and citations for every licensed nursing home. Facilities with a pattern of pressure injury citations, staffing violations, or substantiated complaint investigations have shown the warning signs before. The records are public and free to access.
When families notice the medical signs and feel that the facility’s records or explanations do not match what they are seeing, the next step is usually a request for a full medical record review, sometimes with an outside geriatric specialist or a nursing home abuse lawyer California families consult to understand what the documentation actually shows compared to what the resident’s body shows. The legal review and the medical review tend to surface the same gaps for the same reasons.
The Pattern Ruby’s Case Made Visible
Ruby Evans was 96, immobile, recovering from a stroke, and dependent on her care team to do exactly what her care plan specified. The plan was simple and standard. Reposition every two hours. The execution required staffing the unit at a level that allowed the turns to happen. When the staffing was not there, the turns were missed. When the turns were missed, the wound developed. When the wound was visible, the records were adjusted to suggest care that had not been performed.
That pattern is what the jury saw, and what California’s elder abuse framework was specifically designed to address. The medical signs that something is going wrong almost always show up before the catastrophe does, but only if someone is looking for them, and only if the records can be trusted to reflect what is actually happening in the room.
References:
Vallejo Sun – Jury orders Vallejo care facility to pay $15M in lawsuit over 96-year-old woman’s death (January 15, 2026)
Yahoo News – Solano County jury awards $15.75M to family of senior who died after care center stay (January 14, 2026)
Nursing Home Abuse Center – California Nursing Home Stage 3 Bedsore Wrongful Death Verdict (case summary of Ruby Evans v. Windsor Vallejo Care Center)
California Office of the Attorney General – State of California v. Sweetwater Care (June 2025 lawsuit citing 25,000+ violations and chronic understaffing)
California Welfare and Institutions Code Section 15657 – Elder Abuse and Dependent Adult Civil Protection Act enhanced remedies