
Tibia (Shin Bone): Location, Anatomy and Common Conditions
The tibia is the second largest bone in the human body, and is the main weight bearing bone of the lower leg. It extends from the base of the knee to the ankle, and is attached to the femur and fibula. It is a necessity for standing, walking and maintaining balance.
Detailed Anatomy of the Tibia
Like other long bones, the breaks down into three main sections:
- Proximal end (top)
- Shaft (middle)
- Distal end (bottom)
The Proximal End (Top of the Tibia):
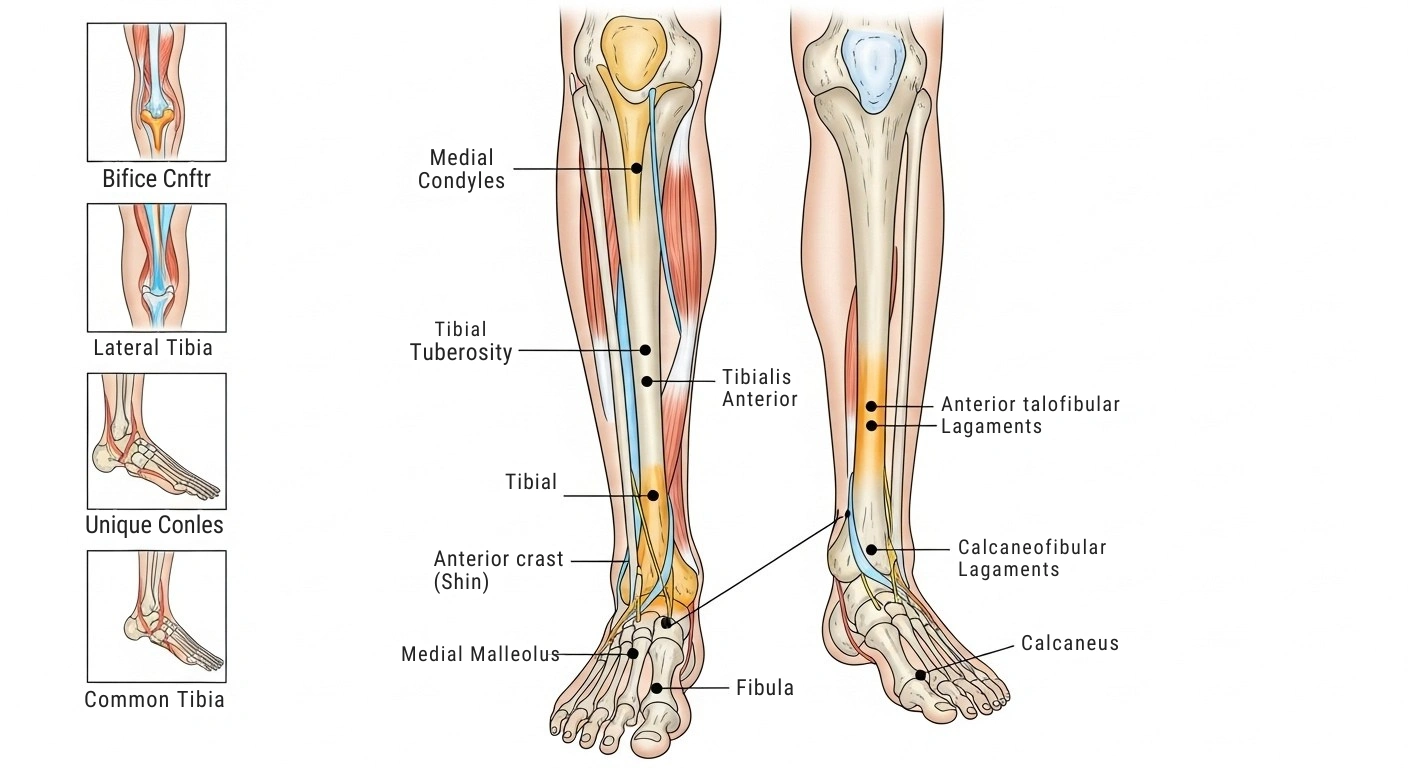
The top part is the widest. It flares out and forms two flat platforms the medial condyle and the lateral condyle. The medial one is slightly larger.
Sitting between the condyles, you’ll find a raised area called the intercondylar eminence, also known as the spine. It sticks up on either side as the medial and lateral intercondylar tubercles. Some doctors refer to the lateral one as the Gerdy tubercle.
The ACL and PCL two key knee ligaments you’ve probably heard about in sports news attach near this area. The menisci connect here too.
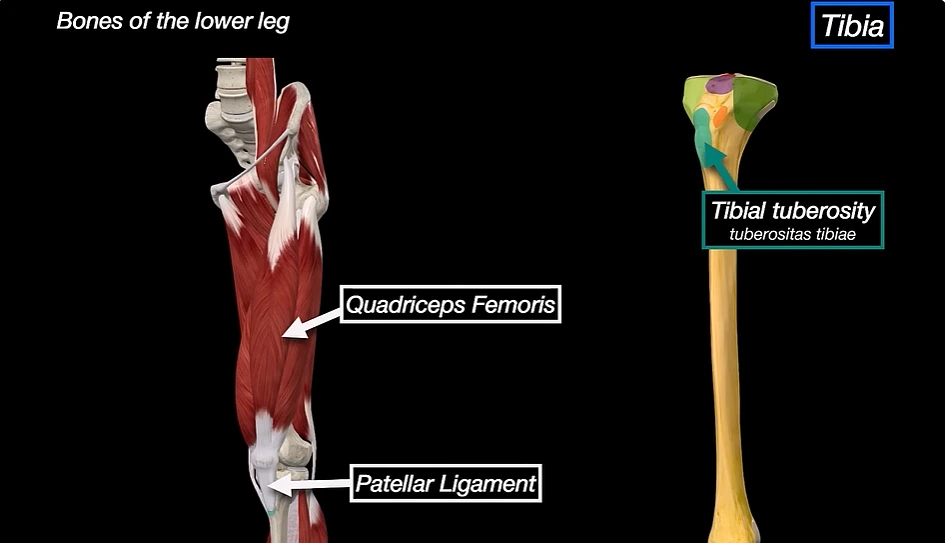
Now, look at the front side just below the condyles. There’s a bump called the tuberosity. You can feel it easily below your kneecap. Your patellar tendon attaches right here, linking your kneecap to your shin bone. This spot works hard every time you straighten your knee walking, jumping, kicking, you name it.
The Shaft (Middle Section):
Three Borders:
- Anterior border — the sharp edge running down the front of your shin. It starts at the tuberosity and goes all the way down. This is the part that takes the hit when you walk into furniture.
- Medial border — runs from the back of the medial condyle down to the medial malleolus.
- Lateral border (interosseous crest) — the interosseous membrane attaches along this edge, holding the fibula together.
Three Surfaces:
- Medial surface — smooth and subcutaneous, meaning it sits right under your skin with almost no muscle on top. You can feel it along the entire length of your leg.
- Lateral surface — muscles from the front compartment of the leg cover this side.
- Posterior surface — features the soleal line, a diagonal ridge where the soleus muscle starts. The flexor digitorum longus and tibialis posterior also begin here.
The Distal End (Bottom of the Tibia):
The bottom end is smaller than the top, and its shape shifts from triangular to more rectangular.
Here are the key landmarks:
- Medial malleolus — that bony bump on the inside of your ankle. It helps keep your ankle joint stable.
- Fibular notch — a groove on the outer side where the fibula fits snugly against.
- Inferior articular surface — the smooth bottom that rests on top of the talus bone.
Joints and Articulations
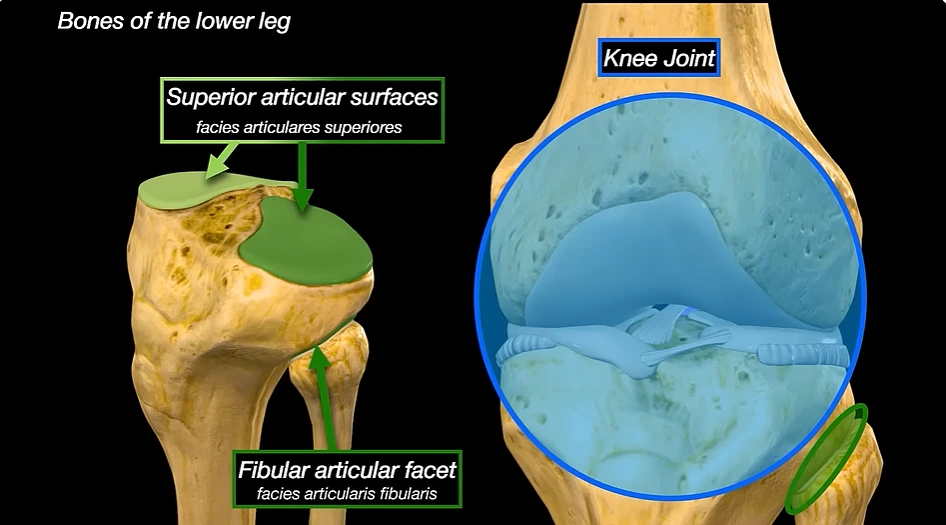
- Knee joint — the proximal meets the femur here. It’s the largest and most complex joint in your body.
- Superior tibiofibular joint — the proximal meets the fibula head. A small synovial joint that allows slight gliding movement.
- Inferior tibiofibular joint — the fibular notch connects with the distal fibula. Strong ligaments hold this fibrous joint together, and it’s essential for ankle stability.
- Ankle joint (talocrural joint) — the distal and medial malleolus sit on the talus. This hinge joint lets you point your foot up and down.
Muscles Attached to the Tibia
Your anchors about 11 muscles. Some start from it, and others end on it.
- Tibialis anterior — comes off the lateral surface and lifts your foot upward.
- Extensor digitorum longus — starts at the lateral condyle and straightens your toes.
- Tibialis posterior — originates from the posterior surface and supports the arch of your foot.
- Soleus — begins at the soleal line. It’s a major calf muscle you use for walking and running.
- Flexor digitorum longus — also starts on the posterior surface and curls your toes downward.
Muscles That Attach:
- Sartorius and gracilis — connect to the medial surface of the proximal.
- Quadriceps femoris — attaches to the tuberosity through the patellar tendon.
- Semimembranosus — connects to the medial condyle.
- Semitendinosus — attaches just below the medial condyle.
- Popliteus — connects along the soleal line on the back surface.
- Tensor fasciae latae — reaches the lateral tubercle through the iliotibial band.
Blood Supply and Nerve Supply
Gets its main blood from the nutrient artery, a branch of the posterior artery. This artery enters through the nutrient foramen on the back surface and feeds the inner two-thirds of the bone.
The outer parts and both ends receive blood from periosteal arteries tiny vessels that run along the periosteum, the thin tissue layer wrapping around the bone.
Bone Development and Ossification
Most guides skip this part, but it matters especially if you’re a parent or a young athlete.
Your doesn’t start out as one solid piece of bone. Instead, it develops through a process called endochondral ossification. Basically, a cartilage model slowly turns into real bone over time.
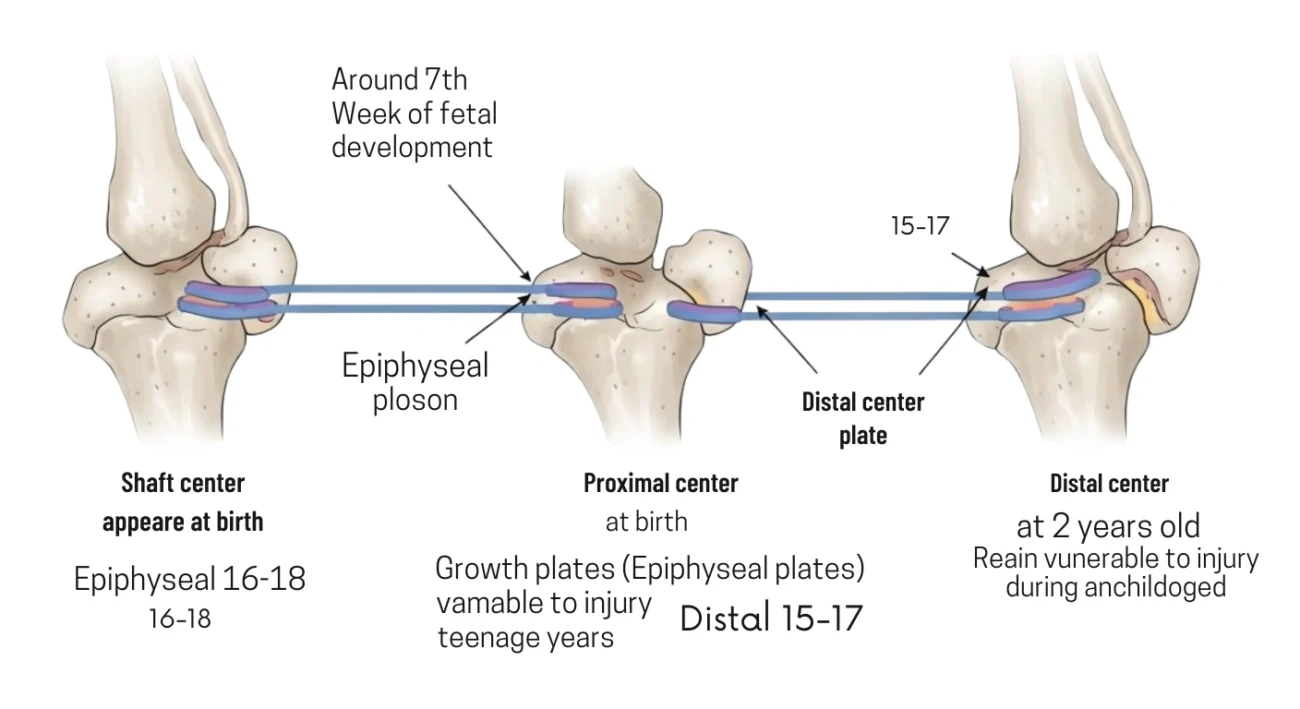
This process kicks off from three separate centers:
- Shaft center — shows up around the 7th week of fetal development.
- Proximal center (top) — appears around the time of birth.
- Distal center (bottom) — appears during the second year of life.
Between these centers sit the growth plates, also called epiphyseal plates. These cartilage zones let the bone grow longer throughout childhood and the teenage years.
The proximal growth plate usually closes around age 16 to 18. The distal one closes around age 15 to 17. Until they close, these areas stay vulnerable to injury. That’s why active kids and teenagers deal with problems like Osgood-Schlatter disease and growth plate fractures more often than adults.
How the Tibia Changes with Aging
Bone density hits its peak around age 30. After that point, your body breaks down old bone a little faster than it builds new bone. For women, this process speeds up a lot after menopause because estrogen levels drop and estrogen plays a big role in protecting bone health.
Over the years, the cortical bone (the hard outer shell) gets thinner. The trabecular bone (the spongy stuff inside the ends) loses density.
The cartilage covering the plateau also wears down with time. That can lead to osteoarthritis in the pain behind knee, bringing pain, stiffness, and less mobility.
But here’s the good news. Staying active, eating calcium-rich foods, getting enough vitamin D, and doing weight-bearing exercises throughout your life can slow all of these changes down.
Common Conditions That Affect
Shaft Fractures:
These rank among the most common long bone fractures out there. They usually happen because of high-energy trauma think car accidents, bad falls, or hard sports collisions.
You’ll know something’s wrong because of severe pain, swelling, trouble putting weight on the leg, and sometimes a visible deformity. Doctors treat stable fractures with a cast. If the bone shifts out of place or breaks through the skin, surgery becomes necessary typically an intramedullary nail (a rod inside the bone) or plates and screws.
Plateau Fractures:
These happen at the very top of the involve the knee joint surface. They’re common after falls from a height or a direct blow to the side of the knee.
Because the joint surface takes the damage, leaving a plateau fracture untreated can cause arthritis and meniscus problems down the road. Many of these fractures need surgery.
Distal Tibial and Ankle Fractures:
Fractures at the bottom of the often affect the ankle too. Two specific types worth knowing:
- Pilon fracture — damages the distal joint surface with the ankle, usually from a high-energy fall.
- Tillaux fracture — affects the growth plate area in teenagers.
Both types typically require surgery to fix properly.
Shin Splints (Medial Tibial Stress Syndrome):
What causes it? The muscles, tendons, and periosteum attached to the get irritated. Overtraining, running on hard surfaces, worn-out shoes, and flat feet or high arches all play a part. Rest, ice, better shoes, and a smarter training plan usually do the trick.
Stress Fractures:
These are tiny cracks in the bone that build up over time from repetitive force not from one single hit. Runners, dancers, and military recruits get them a lot.
The main symptom is a dull ache that gets worse during activity and eases up with rest. Regular X-rays often miss stress fractures early on, so doctors typically order an MRI or bone scan to confirm.
Osgood-Schlatter Disease:
This one mainly hits teenagers going through growth spurts especially those who play sports with lots of running and jumping. It causes pain and swelling right at the tuberosity.
Blount Disease:
Blount disease also targets the growth plate at the top. When too much weight or mechanical stress pushes on it, the inner part of the plate slows down. But the outer part keeps growing normally.
This condition shows up in toddlers (infantile form) and sometimes in teenagers too. Mild cases respond to bracing. Severe cases need surgery.
Paget’s Disease of Bone:
With Paget’s disease, abnormal bone remodeling makes bones bigger, weaker, and more likely to break, the bone can bow outward, causing pain and making it tough to walk. Doctors usually treat it with bisphosphonate medications.
Osteoporosis:
Osteoporosis thins out your bones by reducing their density. Since the bears so much weight, it becomes a prime target for fractures sometimes even from a simple stumble. This condition affects older adults most often, especially women after menopause. A DEXA scan can catch it early.
Osteomyelitis:
Osteomyelitis means a bone infection. It most commonly develops after an open fracture or surgery, when bacteria find their way inside. Symptoms include deep pain, swelling, redness, and fever. Treatment usually involves weeks of antibiotics, and severe cases may need surgery to clean out the infected tissue.
Posterior Tibial Tendinitis:
This happens when the tendon running behind your medial malleolus gets irritated or swollen. You’ll feel pain on the inner side of your ankle. If you ignore it long enough, the arch of your foot can start to weaken.
Compartment Syndrome: A Serious Emergency
This condition deserves its own section because it can be life-threatening, and most people have never even heard of it.
Your lower leg contains four compartments. Tough tissue called fascia wraps around each one. Inside, you’ll find muscles, nerves, and blood vessels.
When a tibial fracture or serious injury causes swelling inside one of these compartments, pressure starts building. Since fascia doesn’t stretch much, the pressure has nowhere to escape. Eventually, it can cut off blood flow to the muscles and nerves inside.
Warning signs you should never ignore:
- Severe pain that seems way worse than the injury itself.
- Tightness and hard swelling in the leg.
- Numbness or tingling in the foot or toes.
- Weakness when you try to move your foot.
- Pain that spikes when someone gently stretches your toes.
The only fix is a fasciotomy a surgery where the surgeon cuts open the fascia to release the pressure. If doctors don’t act within about six to eight hours, the damage can become permanent. We’re talking dead muscle tissue, nerve injury, or in the worst cases, amputation.
The Tibia in Emergency Medicine: Intraosseous Access
When paramedics or ER doctors can’t get an IV line started during cardiac arrest, severe trauma, or shock, for example they turn to a technique called intraosseous (IO) access.
- Proximal, just below the knee the go-to spot.
- Distal, just above the ankle the backup option.
Why does this work? Because the bone marrow has a dense network of veins that feeds directly into your body’s circulation. Fluids, medications, and even blood products delivered this way reach your heart and organs almost as fast as a regular IV.
IO access has become standard practice in emergency medicine. It has saved countless lives in situations where every second counts.
How Doctors Diagnose Tibia Problems
It all starts with a physical exam. Your doctor will check for swelling, tenderness, any deformity, and how well you can move the leg. They’ll also look for signs of compartment syndrome.
After the exam, imaging usually comes next:
- X-rays — the go-to first step for spotting most fractures and bone problems.
- MRI — the best option for stress fractures and soft tissue injuries that X-rays miss.
- CT scan — helpful for complex fractures, especially plateau breaks, when doctors need to plan surgery.
- Bone scan — picks up infections and metabolic bone diseases like Paget’s.
- DEXA scan — measures bone density and helps diagnose osteoporosis.
Treatment and Rehabilitation
Conservative Treatment:
For milder issues like shin splints and early stress fractures, the plan usually includes rest, ice, anti-inflammatory medications, and a slow return to activity.
Surgical Treatment:
More serious fractures may need one of these approaches:
- Intramedullary nailing — a metal rod goes inside the bone’s canal to hold everything in place.
- Plate and screw fixation — hardware goes on the outside of the bone.
- External fixation — a frame sits outside the leg, connected to the bone through pins.
- Fasciotomy — emergency surgery for compartment syndrome.
Physical Therapy and Rehabilitation:
- Getting your range of motion back in the knee and ankle.
- Rebuilding strength in the surrounding muscles.
- Improving balance and coordination.
- Gradually working your way back to walking, running, and sports.
Starting to move early safely and with guidance helps prevent stiffness, muscle loss, and blood clots. Most tibial fractures take anywhere from 12 weeks to 6 months to heal fully, depending on how bad the break was and what treatment you needed