
Tirzepatide: How It’s Used & Side Effects

Everything below is general information, not medical advice. This is a prescription Health Medicines, and whether it’s right for you and how to use it safely is a conversation for you and your doctor, not a blog post. People respond differently to medications, drug labels get updated, and new research comes out all the time. If something here sparks a question about your own care, take it to a clinician who knows your full history. And if you’re dealing with a medical emergency, please skip the article and call your local emergency services.
Key Takeaways
- This is the first FDA-approved drug that activates two gut-hormone receptors at once (GIP and GLP-1). You’ll see it sold under two brand names Mounjaro for type 2 diabetes and Zepbound for weight management and obstructive sleep apnea.
- It’s a once-weekly injection, taken on the same day each week, started low and slowly increased to keep stomach side effects manageable.
- In major trials, people lost roughly 20–25% of their starting body weight at the highest doses, and people with type 2 diabetes saw substantial drops in HbA1c.
- The most common side effects are gut-related nausea, vomiting, diarrhea, constipation and they usually settle down after the first few weeks.
- Serious risks are rarer but real: pancreatitis, gallbladder problems, kidney issues from dehydration, and a boxed warning about thyroid tumors seen in animal studies.
- It’s not for everyone. People with certain thyroid cancers in the family, pregnant women, and those with severe stomach-emptying problems should steer clear.
What Is Tirzepatide?
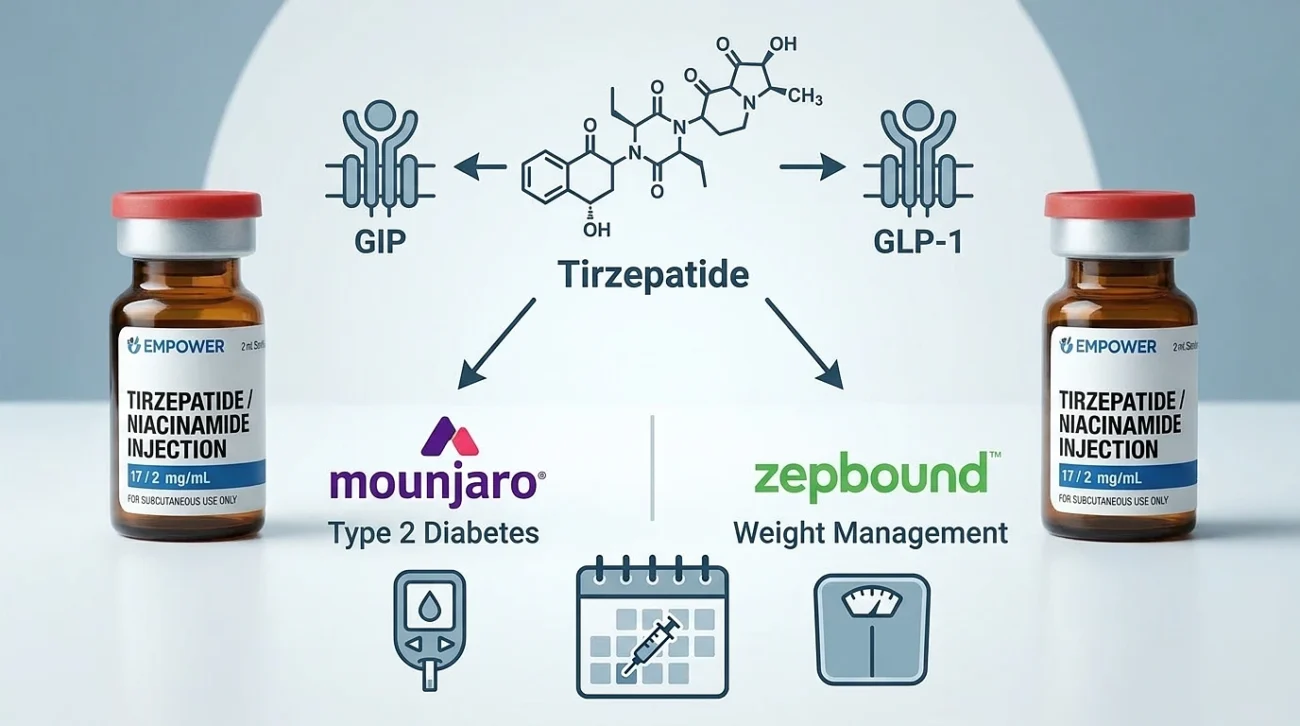
Tirzepatide is a lab-made peptide that mimics two hormones your gut releases naturally after a meal: GIP (glucose-dependent insulinotropic polypeptide) and GLP-1 (glucagon-like peptide-1). Both nudge the body toward better blood-sugar control and reduced appetite, but in slightly different ways. Older drugs in this space semaglutide and liraglutide only hit GLP-1. The newer dual-action approach hits both, and that combination seems to make a real difference.
The FDA approved it for type 2 diabetes in May 2022, and then for chronic weight management in November 2023. Eli Lilly sells the same active ingredient under two names depending on what it’s prescribed for:
- Mounjaro – for type 2 diabetes.
- Zepbound – for chronic weight management, and (more recently) for moderate-to-severe obstructive sleep apnea in adults with obesity.
The molecule itself has a fatty acid tail that lets it cling to a protein called albumin in the bloodstream. That clinginess is what stretches its half-life out to about five days, which is why one injection per week is enough.
How It Works Tirzepatide
The drug doesn’t do just one thing. It works through several overlapping mechanisms.
It tells your pancreas to release more insulin, but only when your blood sugar is actually rising so it’s not constantly flooding your system. At the same time, it dials down glucagon, the hormone that signals your liver to dump stored sugar into the blood. That alone takes the edge off post-meal sugar spikes.
It also slows down how quickly your stomach empties, which keeps you feeling full longer and smooths out the glucose rollercoaster after meals. And it acts on appetite centers in the brain, dampening hunger signals before you even sit down to eat.
There’s emerging evidence that the GIP component improves how fat tissue handles incoming nutrients too, which may be part of why this dual-acting therapy outperforms GLP-1-only drugs head-to-head.
What It’s Approved For
Type 2 diabetes is the original indication. Mounjaro is added to diet and exercise to bring blood sugar under better control, either on its own or alongside other diabetes medications.
Chronic weight management is the indication that put this drug on every front page. Zepbound is approved for adults whose BMI is 30 or higher, or 27 or higher with at least one weight-related condition like high blood pressure, high cholesterol, type 2 diabetes, heart disease, or sleep apnea.
Obstructive sleep apnea Zepbound is also approved for moderate-to-severe OSA in adults with obesity, used alongside diet and exercise.
Beyond the official approvals, researchers are looking hard at this molecule for fatty liver disease (NASH/MASH), heart failure, PCOS, and even certain inflammatory skin conditions. Those uses are still in the research phase and aren’t approved yet.
How It’s Actually Used
The medication comes as a subcutaneous injection meaning the needle goes just under the skin, into the fatty layer in your stomach, thigh, or upper arm. You rotate sites week to week to avoid irritation.
The injection is once weekly, on whichever day works best for you, with or without food. Pick a day, stick with it. If you forget, you generally have a four-day window to take it; miss that, and you skip the dose and go back to your regular schedule the following week.
The dose climbs slowly. Almost everyone starts at 2.5 mg for the first four weeks that’s the “warm-up” dose, not a maintenance dose. From there, your prescriber bumps it up every four weeks if you’re tolerating it:
| Weeks | Dose |
|---|---|
| 1–4 | 2.5 mg (starting only) |
| 5–8 | 5 mg |
| 9–12 | 7.5 mg |
| 13–16 | 10 mg |
| 17–20 | 12.5 mg |
| 21+ | 15 mg (maximum) |
Plenty of people don’t need to climb all the way to 15 mg. Many do well at 5 or 10 mg, and the goal is the lowest dose that gets the job done.
A practical note on storage: keep the pens in the fridge, between 2 and 8°C. They tolerate room temperature for a limited time if you’re traveling, but never freeze them and never leave them in direct sun.
What the Research Actually Shows
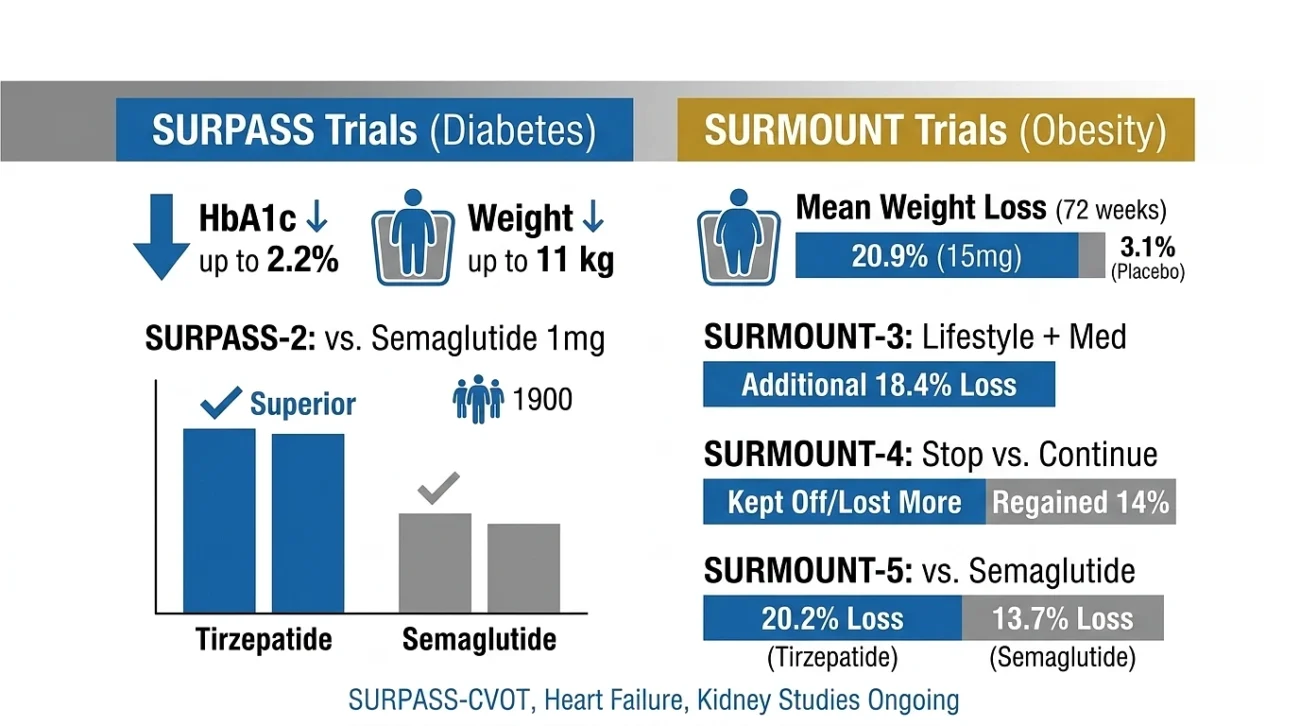
This treatment didn’t get its reputation by accident. Two big trial programs built the case for it: SURPASS for diabetes and SURMOUNT for obesity.
In SURPASS, the medication consistently lowered HbA1c by up to about 2.2 percentage points and dropped body weight by as much as 11 kilograms, all with a tolerability profile most patients could live with. The SURPASS-2 trial put it head-to-head against semaglutide 1 mg in nearly 1,900 people with type 2 diabetes and the dual-receptor agonist came out ahead at every dose tested.
The SURMOUNT trials were the headline-makers:
- SURMOUNT-1 showed roughly 20.9% mean weight loss at 72 weeks on the 15 mg dose, compared to about 3.1% on placebo.
- SURMOUNT-3 combined an intensive lifestyle program with the medication and saw an extra 18.4% weight loss after randomization, while the placebo group actually regained a bit.
- SURMOUNT-4 answered a question a lot of people were quietly worrying about: what happens when you stop? The answer wasn’t comforting. People who stopped regained around 14% of their body weight, while those who stayed on it not only kept the weight off but lost a little more.
- SURMOUNT-5, the first direct comparison against semaglutide for weight loss, showed about 20.2% weight reduction with the dual-hormone drug versus about 13.7% with semaglutide over 72 weeks.
There’s also a major cardiovascular outcomes trial called SURPASS-CVOT still running, along with studies in heart failure and kidney disease. The full picture of long-term benefit and risk is still coming into focus.
The Side Effects
Let’s be honest about this part: side effects are real, and most of them live in your stomach. The good news is that they tend to be worst during the dose-escalation phase and ease up as your body adjusts.
In a large analysis of what users actually report, the most common complaints are nausea (by far the leader, mentioned by roughly a third of users), fatigue, vomiting, constipation, diarrhea, and a generally smaller appetite. Heartburn, burping, and mild abdominal discomfort show up too. Injection-site reactions a bit of redness or itching happen but are usually minor.
Hair thinning sometimes gets blamed on the medication, but it’s more often a side effect of the rapid weight loss itself. The body doesn’t love losing 20% of its mass in under a year, and hair is one of the first things to protest.
A few things genuinely help: smaller meals, going easy on greasy or fried food, drinking enough water, and slowing dose increases if your stomach is staging a revolt. There’s no medal for racing to 15 mg.
The Serious Stuff Worth Knowing About

Most adverse events are mild. But this drug carries some warnings that aren’t decorative.
- Thyroid C-cell tumors – In rodent studies, drugs in this class caused thyroid tumors. Whether that translates to humans isn’t fully clear, but it’s enough that anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 syndrome should not use it. This is a hard line, not a soft caution.
- Pancreatitis – If you develop severe abdominal pain that doesn’t quit, especially pain that travels to your back, that’s a stop-and-call-your-doctor situation.
- Gallbladder disease – Gallstones and gallbladder inflammation have shown up, partly because rapid weight loss itself raises that risk.
- Severe GI events – Rare but documented: gastroparesis (where the stomach essentially stops emptying), ileus, and bowel obstruction. People with pre-existing severe gastroparesis shouldn’t take it.
- Low blood sugar – On its own, the medication rarely causes hypoglycemia. Combine it with insulin or sulfonylureas, though, and the risk goes up sharply. Doses of those medications often need to come down.
- Kidney injury – Usually a downstream effect of dehydration from vomiting or diarrhea. Hydration matters more than people think.
- Eye issues in diabetes – Rapid blood-sugar improvements can temporarily worsen diabetic retinopathy. People with eye disease need ongoing monitoring.
- Allergic reactions – Rare, but anaphylaxis and angioedema have been reported. Skin reactions overall are roughly in line with other drugs in the class.
- Mood changes – Zepbound’s labeling specifically cautions against use in people with a history of suicidal thoughts or attempts. Any new or worsening mood symptoms should go straight to your prescriber.
- Pregnancy and contraception – Don’t use it during pregnancy. And there’s a wrinkle worth knowing: because the drug slows stomach emptying, it can interfere with how oral birth control is absorbed. If that’s your method, you’ll want backup contraception or a non-pill option for at least four weeks after starting and after each dose increase.
Drug Interactions and Practical Considerations
Because the medication slows down digestion, it can change how other oral drugs get absorbed. That mostly matters for birth control pills (covered above) and any medication where the dose has to be precise anticoagulants, certain seizure medications, and a few others. Before you start, walk your prescriber through everything you take, including supplements.
Who Shouldn’t Take It
The clear “no” list:
- Personal or family history of medullary thyroid carcinoma or MEN 2 syndrome.
- Known serious allergic reaction to the active ingredient.
- Pregnancy or active plans to become pregnant.
- Severe gastroparesis.
The “talk carefully with your doctor first” list:
- History of pancreatitis.
- Severe GI disease.
- History of suicidal thoughts or attempts (especially for Zepbound).
Older adults and people with kidney or liver issues can often still use it, but they need closer monitoring.
Practical Tips If You are Starting
Pick a weekly day and lock it in with a phone alarm. Consistency beats which day you pick.
Rotate injection sites don’t keep poking the same spot, your skin will let you know.
Eat slowly, and stop sooner than you think you should. The drug already nudges your appetite down; meeting it halfway makes a difference.
Keep your protein up. Rapid weight loss without enough protein eats into muscle, and you don’t want that.
Track how you feel. A simple note on your phone symptoms, weight, mood turns vague impressions into useful data for your appointments.
And don’t stop the medication on a whim. The data on what happens after stopping is sobering: most of the weight comes back unless other changes are firmly in place.
References
- Sun B, Willard FS, Feng D, et al. Adverse events related to the dual GIP/GLP-1 agonist therapy. Journal of Clinical & Translational Endocrinology. 2023. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9915969/
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Once-weekly therapy for the treatment of obesity (SURMOUNT-1). New England Journal of Medicine. 2022;387(3):205–216.
- Frías JP, Davies MJ, Rosenstock J, et al. Dual GIP/GLP-1 receptor agonist versus semaglutide once weekly in patients with type 2 diabetes (SURPASS-2). New England Journal of Medicine. 2021;385(6):503–515.
- Wadden TA, Chao AM, Machineni S, et al. Continued treatment after intensive lifestyle intervention in adults with overweight or obesity: the SURMOUNT-3 phase 3 trial. Nature Medicine. 2023. https://www.nature.com/articles/s41591-023-02597-w
- Aronne LJ, Sattar N, Horn DB, et al. Continued treatment for maintenance of weight reduction in adults with obesity: the SURMOUNT-4 randomized clinical trial. JAMA. 2024. https://pubmed.ncbi.nlm.nih.gov/38078870/
- Aronne LJ, Horn DB, le Roux CW, et al. SURMOUNT-5: head-to-head comparison with semaglutide in adults with obesity. New England Journal of Medicine. 2025.
- Chen X, Zhang J, et al. Innovative applications in type 2 diabetes management and future prospects in cardiovascular health. 2024. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11387164/
- El-Amawy HS. Cutaneous adverse events, emerging therapeutic roles, and cosmetic implications of dual incretin therapy in dermatology. Anais Brasileiros de Dermatologia. 2025. DOI: 10.1016/j.abd.2025.501255
- Karagiannis T, Avgerinos I, Liakos A, et al. Safety and effectiveness in obesity without type 2 diabetes mellitus. Cureus. 2024. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10844768/
- Self-reported side effects of semaglutide and dual incretin therapy in online communities a cross-sectional analysis of Reddit data. Preprint, arXiv. 2025.
- US Food and Drug Administration. Mounjaro prescribing information. Eli Lilly and Company. Updated 2024.
- US Food and Drug Administration. Zepbound prescribing information. Eli Lilly and Company. Updated 2024.
- Eli Lilly and Company. Investor news release: significant and superior weight loss results from two pivotal studies. https://investor.lilly.com/news-releases/news-release-details/tirzepatide-demonstrated-significant-and-superior-weight-loss