How to Release a Pinched Nerve in Shoulder Blade

You know that pain. The zinging pain deep beneath your shoulder that’s refusing to be banished, despite all your stretching, massaging and contortions. Maybe it tingles. Maybe it throbs. And, every time you try to massage it away, it will feel better for a while, only to reappear ten minutes later.
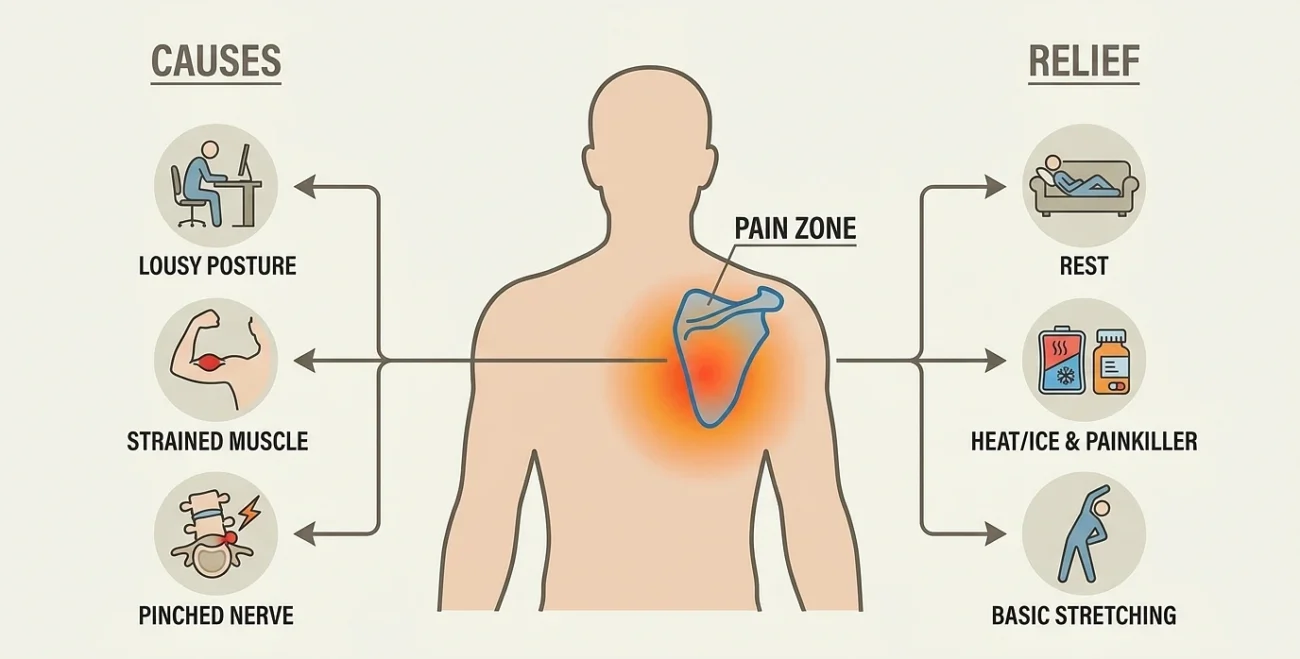
Here’s the part most people don’t know: the pain isn’t actually coming from your shoulder blade.
In nearly every case, what you’re feeling is a nerve being pinched up in your neck. The pain just travels along the nerve and lands wherever it goes often right between your shoulder blade and spine. The medical name is cervical radiculopathy. Most people just call it a pinched nerve.
This is also why massaging the painful spot doesn’t really fix anything. You’re chasing the symptom, not the cause. The actual compression is happening up at C5, C6, or C7 the lower part of your neck. C7 is the most common offender, with C6 right behind it. Until you take pressure off the nerve at the source, it’ll keep flaring up.
This is a more common issue than you might think. The Mayo Clinic’s Rochester study found cervical radiculopathy at 83 per 100,000 each year, with the biggest increase between the ages of 50 and 54 (Radhakrishnan et al., Brain, 1994). It’s becoming more common, largely due to modern life. Hansraj’s famous biomechanics study calculated how much strain is put on your neck when you bend your head forward to look at your phone. The weight of an average head is 10-12 pounds. Once you tilt down 15 degrees, the strain on your neck becomes 27 pounds. Tilt 30 degrees, you’re at 40. At 60 degrees, the position many of us hunch forward at, your head weighs 60 pounds (Hansraj, Surgical Technology International, 2014). That’s like an 8-year-old on your shoulders while browsing Facebook.
How to Tell If It’s Actually a Pinched Nerve
Before you start treating anything, make sure you’re treating the right thing. A muscle knot, a rotator cuff strain, and a pinched nerve all hurt in the same general neighborhood, but each one needs a completely different approach. Treat the wrong one and nothing changes.
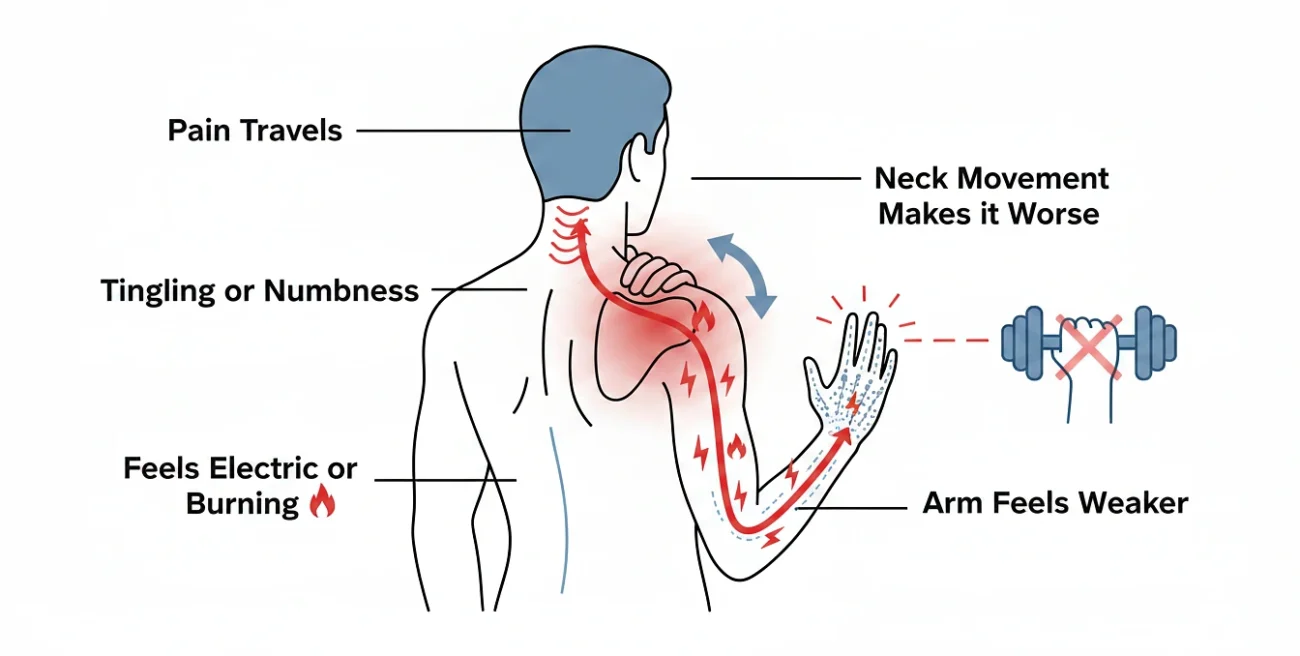
A pinched nerve has a distinct fingerprint:
- The pain travels. It doesn’t sit still in one place. It shoots from your neck into the shoulder blade, sometimes running down the arm into your hand or fingers.
- You feel tingling or numbness. This is the dead giveaway. Muscles don’t tingle. Nerves do.
- It feels electric or burning. Not the dull ache of a tight muscle. Sharper, hotter, almost buzzy.
- Neck movement makes it worse. Turn your head toward the sore side, or tip it back, and the pain spikes.
- Your arm feels weaker. Grip might feel off. Lifting overhead might suddenly feel awkward.
Doctors confirm it with a couple of quick physical tests the Spurling test (gentle downward pressure on a tilted head) and the upper limb tension test. Both reproduce the symptoms when there’s actual nerve compression (Childress & Becker, American Family Physician, 2016).
If your pain is just a deep, dull ache parked in the muscle near your shoulder blade no tingling, no shooting, no weakness that’s likely a trigger point, not a pinched nerve. Different beast, different fix.
The First 48 Hours
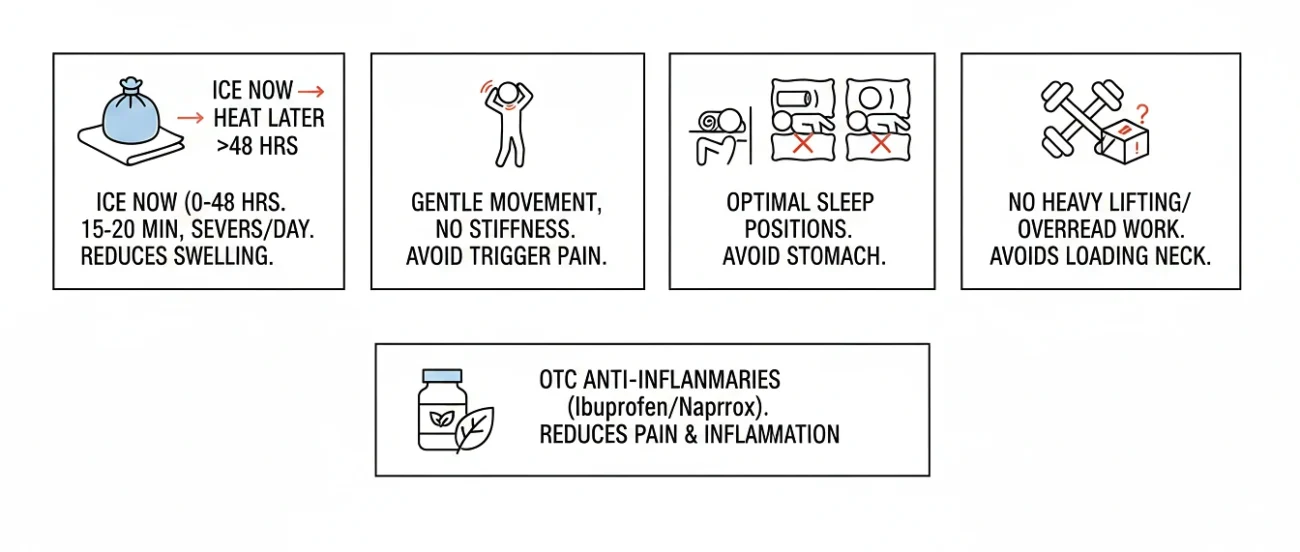
The first two days are damage control. Bring the inflammation down, avoid making things worse.
- Ice now, heat later. For the first 48 hours, ice is your friend. Wrap a cold pack in a thin towel and rest it on the base of your neck and upper shoulder for 15 to 20 minutes at a time, several times a day. The cold tames the swelling pressing on the nerve. After two days, switch to heat it loosens the surrounding muscles and pulls fresh blood into the area.
- Rest, but don’t lock up. Lying flat for three days is a mistake. Stiff necks always end up worse. Move gently, just steer clear of whatever specifically triggers the sharp pain.
- Sleep position actually matters. Side sleepers need a pillow that keeps the neck level with the spine. Stomach sleeping is the worst possible setup your neck is rotated for hours. If that’s your default position, this is the time to break the habit, at least until the pain settles. Back sleepers should slip a small rolled towel under the curve of the neck for support.
- Skip the heavy and overhead stuff. Grocery bags, ceiling painting, weight training all off-limits for now. Loading the neck keeps the nerve angry.
- OTC anti-inflammatories help. Ibuprofen and naproxen knock down both pain and inflammation, and they’re recommended right at the top of clinical guidelines (Childress & Becker, American Family Physician, 2016). Stick to label dosing, and check with your doctor first if you’ve got stomach, kidney, or heart issues.
The Stretches That Actually Work
Once you’re past the worst 2 or 3 days, gentle movement is what does the real work. But here’s the key thing most people miss: you’re not stretching the painful spot. You’re opening up the space in your neck where the nerve is being squeezed. Different target, different result.
Move slowly. If anything makes the radiating pain or tingling worse, stop. That’s a warning, not progress.
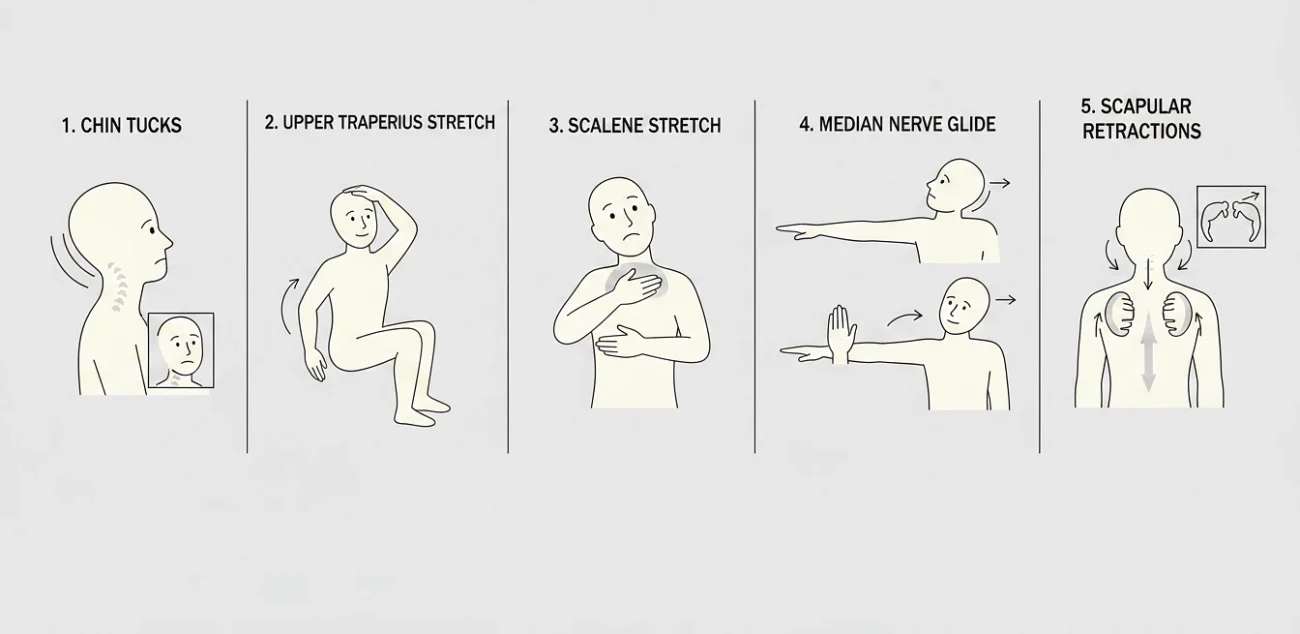
1. Chin Tucks
If you only do one move, do this one. It directly counteracts the forward-head slump that drives most pinched nerves in the upper body.
- Sit or stand tall, shoulders relaxed.
- Without tilting your head up or down, slide your chin straight back. Like you’re trying to make the worst double chin you can.
- Hold 5 seconds. Release.
- 10 reps, 3 to 5 times a day.
You should feel a soft pull at the base of your skull. Stick with it and chin tucks gradually pull your head back where it belongs over your shoulders, not in front of them.
2. Upper Trapezius Stretch
This loosens that thick rope of muscle running from your neck to the top of your shoulder, which is almost always tight when there’s a pinched nerve in play.
- Sit upright. Slip your right hand under your right thigh this anchors the shoulder so it can’t sneak up.
- With your left hand, gently pull your head toward your left shoulder.
- Hold 30 seconds. Switch sides.
- Do 2 to 3 sets per side.
3. Scalene Stretch
The scalenes are the strappy muscles running along the side of your neck. When tight, they compress the nerves heading down into your shoulder.
- Sit tall. Right hand on your collarbone, holding it down gently.
- Tilt your head back and to the left, eyes slightly upward.
- Hold 20 to 30 seconds. Switch sides.
4. Median Nerve Glide (“Nerve Flossing”)
This one sounds odd but it’s brilliant. Physical therapists use it to mobilize the nerve through its sheath kind of like flossing it loose. A 2017 systematic review found nerve gliding produced real, measurable improvements in pain and function for people with cervical radiculopathy (Basson et al., Journal of Orthopaedic & Sports Physical Therapy, 2017).
- Stand with your arm out to the side at shoulder height, palm facing down.
- Bend your wrist back so your fingers point up. Tilt your head toward the opposite shoulder.
- Then flip your palm up and tilt your head toward the same shoulder.
- Alternate slowly, 10 reps. Do this 2 to 3 times a day.
A mild pulling sensation is fine. Sharp pain shooting down your arm means you’ve gone too far pull the range back.
5. Scapular Retractions
When the muscles in your mid-back are weak, your shoulders roll forward, which crushes nerves at the front of the neck. This rebuilds them.
- Sit or stand tall.
- Squeeze your shoulder blades together and down, like you’re trying to pinch a pencil between them.
- Hold 5 seconds. Release.
- 15 reps, 2 to 3 times a day.
When to Stop and See a Doctor
Most pinched nerves clear up within 4 to 6 weeks of solid home care. But certain signs mean stop self-treating and get evaluated.
Don’t wait if any of these show up:
- The pain keeps getting worse after a week of consistent care.
- You’re losing strength. Grip slipping, arm feeling weak, hand feeling clumsy.
- The numbness is spreading down your arm or into your fingers.
- Loss of bowel or bladder control. This is a medical emergency. Go to the ER, no exceptions.
- The pain followed a fall, accident, or any kind of impact.
- It’s been more than 6 weeks with no improvement despite consistent rest, stretching, and posture work.
Your doctor may order an MRI to check for a herniated disc or bone spur. From there, the usual path is physical therapy, sometimes a steroid injection, and rarely really rarely surgery. Surgical treatment is reserved for cases that haven’t responded after 6 to 12 weeks or where there’s clear, progressing nerve damage.
References
- Radhakrishnan, K., et al. Epidemiology of cervical radiculopathy: A population-based study from Rochester, Minnesota, 1976 through 1990. Brain, 1994.
- Childress, M. A., & Becker, B. A. Nonoperative Management of Cervical Radiculopathy. American Family Physician, 2016.
- Hansraj, K. K. Assessment of Stresses in the Cervical Spine Caused by Posture and Position of the Head. Surgical Technology International, 2014.
- Basson, A., et al. The Effectiveness of Neural Mobilization for Neuromusculoskeletal Conditions: A Systematic Review and Meta-analysis. Journal of Orthopaedic & Sports Physical Therapy, 2017.
- Cervical Radiculopathy (Pinched Nerve) OrthoInfo, American Academy of Orthopaedic Surgeons.
- Pinched Nerve – National Institute of Neurological Disorders and Stroke (NIH).